RESEARCH ARTICLE
Hippokratia 2022, 26(1): 19-24
Zhou X1, Yi F2, Peng L1, Jiang J1, Lan L1
1Department of Nephrology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, 2Department of Nephrology, The Lu’an Hospital Affiliated to Anhui Medical University, The Lu’an People’s Hospital, Lu’an, Anhui, China
![]()
Abstract
Background: Patients with end-stage renal disease are prone to develop heart failure (HF). The N-terminal pro-brain natriuretic peptide (NT-proBNP, BNP) is regarded as the gold standard for diagnosing HF. However, its prognostic sensitivity in patients with end-stage renal disease is sub-optimal. Soluble suppression of tumorigenesis-2 (sST2) has been well studied in HF but rarely in patients with maintenance hemodialysis (MHD). This study aimed to evaluate the value of sST2 in predicting HF in MHD patients.
Methods: Twenty-three patients with New York Heart Association (NYHA) class III-IV were included in the HF group and 88 NYHA class I-II patients in the non-heart failure (NHF) group. sST2 and laboratory indexes were compared between the two groups.
Results: The HF group, compared with the NHF group, presented with higher sST2, more advanced age, higher incidence of coronary heart disease (CHD), left ventricle end-diastolic diameter (LVEDD), and pulmonary artery pressure (PAP), and unchanged parathyroid hormone (iPTH). The HF group also had lower ejection fraction (EF), uric acid, inorganic phosphorus, 25-OH VitD3, and serum albumin. Multivariate logistic regression indicated that age, BNP, and sST2 were independent risk factors of HF in MHD patients. Spearman analysis defined that sST2 was positively correlated with PAP (r =0.283, p =0.003) and C-reactive protein (r =0.354, p <0.001); and negatively correlated with sex (r =-0.255, p =0.007), albumin (r =-0.366, p <0.001), uric acid (r =-0.213, p =0.025), 25-OH VitD3 (r =-0.216, p =0.04), calcium (r =-0.219, p =0.021), and inorganic phosphorus (r =-0.256, p =0.007). Receiver operating characteristic curve analysis determined a positive association between BNP and sST2 (r =0.373, p <0.001), with the area under the curve (AUC) of BNP being 0.822 (sensitivity: 0.783, specificity: 0.830) and the AUC of sST2 being 0.841 (sensitivity: 0.913, specificity: 0.761). The AUC of sST2 was 0.841, and the cut-value was 42.840 (sensitivity: 0.913, specificity: 0.761).
Conclusion: sST2 can predict HF in MHD patients and facilitate early diagnosis and prevention of HF in MHD patients. HIPPOKRATIA 2022, 26 (1):19-24.
Keywords: Soluble suppression of tumorigenesis-2, sST2, N-terminal pro-brain natriuretic peptide, NT-proBNP, hemodialysis, heart failure
Corresponding authors: Lei Lan, and Jun Jiang, Department of Nephrology, The First Affiliated Hospital of University of Science and Technology of China, University of Science and Technology of China, No 17 Lujiang Road, 230001 Hefei, P.R. China, e-mail: lanlei1976@126.com & j361527372@126.com
Introduction
Despite improved survival in chronic kidney disease (CKD) patients, especially those with end-stage renal disease (ESRD), cardiovascular disease (CVD) is the leading cause of death. The secretion of N-terminal pro-brain natriuretic peptide (NT-proBNP, BNP) by cardiomyocytes can be stimulated by stress or volume overload1. NT-proBNP is regarded as the gold standard for diagnosing heart failure (HF)2,3; however, its sensitivity in patients with end-stage renal disease is sub-optimal. Therefore, more favorable indicators are required. Suppression of tumorigenicity 2 (ST2) has two forms: soluble ST2 (sST2) and ST2 ligand (ST2L). sST2 is a prognostic marker of congestive HF4 and, thus, may be an effective diagnostic marker for HF in ESRD. The ligand of ST2 is interleukin 33 (IL-33), which binds to the receptor to produce nuclear signaling and immune regulation in the heart4. The binding of IL-33 to ST2L can induce activation of mitogen-activated protein kinase and nuclear factor signaling pathways in target cells while the binding of IL-33 to sST2 can block this effect5. Early studies determined that sST2 could not be used as a diagnostic marker for CKD6. Moreover, relatively few studies in assessing the outcome of CKD, especially cardiovascular outcomes, have focused on the value of sST2. However, sST2 plays a vital role in the prognosis of all-cause mortality and cardiovascular events in peritoneal dialysis patients7. There are only a few studies on the correlation between the clinical outcome of ESRD patients on hemodialysis and sST28,9. Recently, sST2 has been identified as an independent predictor of all-cause and cardiovascular death in maintenance hemodialysis (MHD) patients10. Therefore, this study aimed to evaluate the value of sST2 alone or in combination with BNP in predicting HF in MHD patients.
Material and methods
Patients
One hundred eleven hemodialysis patients (66 males and 45 females) were included in this study at the Department of Nephrology, First Affiliated Hospital of the University of Science and Technology of China, from October 2020 to October 2021. Twenty-three patients with severe symptoms classified as New York Heart Association (NYHA) class III-IV were included in the HF group, and 88 patients with NYHA class I-II symptoms were included in the non-heart failure (NHF) group11. The average age was 58.83 ± 15.96 years. Hemodialysis patients excluded from the study were patients with chest tightness, asthma, or infectious complications, under 18 years old, had dialysis vintage <3 months, or were non-compliant with the dialysis regimen. The Ethics Committee of Anhui Provincial Hospital approved this study (No 2021-RE-143).
Methods
We retrospectively collected the following patients’ demographics and clinical characteristics: age, sex, hemodialysis time, diabetes history, coronary heart disease history (CHD), left ventricle end-diastolic diameter (LVEDD), ejection fraction (EF), pulmonary artery pressure (PAP), creatine phosphokinase-isoenzyme-MB (CK-MB), sST2, BNP, C-reaction protein (CRP), uric acid, alkaline phosphatase (AKP), calcium (Ca), inorganic phosphorus (P), 25-OH VitD3, albumin and intact parathyroid hormone (iPTH) after hospitalization and before treatment. The general indicators and laboratory indexes were compared between the two groups.
Statistical analysis
We implemented t-tests or Mann-Whitney U-tests to analyze the relationship between continuous variables and sST2, and we present them as means ± standard deviation or medians with the 25th and 75th percentiles, respectively. Qualitative variable analyses were performed using χ2 test. We performed univariate and multivariate logistic regression analyses to identify risk factors of HD in MHD and Spearman analyses to state the correlation between variables and sST2. We used receiver operator characteristic (ROC) curves to assess the accuracy of sST2 and BNP in diagnosing HF in MHD patients. A p-value <0.05 was considered statistically significant.
Results
Clinical characteristics of MHD patients in the HF and NHF groups
The average age was 58.83 ± 15.96 years, and the incidence of HF was 20.72 %. Compared with the NHF group, the HF group presented with higher sST2 (p <0.001), age (p =0.001), incidence of CHD (p =0.038), LVEDD (p =0.023), and PAP (p =0.007), and unchanged iPTH (p =0.931). The HF group also had lower EF (p =0.017), uric acid (p =0.020), P (p =0.019), 25-OH VitD3 (p =0.029), and serum albumin (p =0.011), seen in Table 1.
Univariate and multivariate logistics regression analysis to identify independent predictors of HF in MHD patients
Univariate logistic regression analysis indicated that age, history of CHD (p =0.044), LVEDD (p =0.029), EF (p =0.003), PAP (p =0.001), albumin (p =0.012), uric acid (p =0.023), P (p =0.023), BNP (p <0.001), and sST2 (p =0.000) were correlated to HF (Table 2). When the above indicators were incorporated into multivariate logistic regression analysis, age (p =0.010), BNP (p =0.008), and sST2 (p =0.008) were seen as independent risk factors of HF in MHD patients, seen in Table 2.
The association between variables and sST2
Upon univariate linear regression analysis, a positive correlation was found between sST2 and PAP (r =0.283, p =0.003) or CRP (r =0.354, p <0.001), a negative correlation was found between sST2 and sex (r =-0.255, p =0.007), albumin (r =-0.366, p <0.001), uric acid (r =-0.213, p =0.025), 25-OH VitD3 (r =-0.216, p =0.040), calcium (r =-0.219, p =0.021), and inorganic phosphorus (r =-0.256, p =0.007) (Table 3). Furthermore, positive association between BNP and sST2 was significant (r =0.373, p <0.001) (Table 3). When the above indicators were incorporated into multivariate-adjusted linear regression analysis, albumin was independently associated with sST2 (r =-2.749, p=0.007).
ROC curve analysis of BNP and sST2 in MHD patients
Table 4 and Figure 1 show the results of the ROC curve analysis. The area under the curve (AUC) of BNP was 0.822, with the sensitivity and specificity being 0.783 and 0.830, respectively. The AUC of sST2 was 0.841, with the cut-value of sST2 being 42.840 and the sensitivity and specificity being 0.913 and 0.761, respectively. The AUC of sST2 combined with BNP was 0.892, with the cut-value of sST2 being 55.71 and that of BNP being 35,000, the sensitivity and specificity being 0.957 and 0.795 (Figure 2).
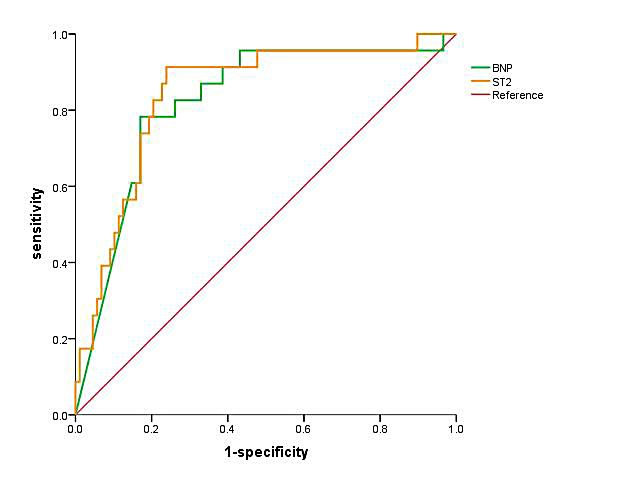
Figure 1: Receiver operator characteristic (ROC) curve analysis of N-terminal pro-brain natriuretic peptide (BNP) [area under the curve (AUC): 0.822, sensitivity: 0.783, specificity: 0.830] and soluble suppression of tumorigenesis-2 (sST2) (AUC: 0.841, sensitivity: 0.931, specificity: 0.761) respectively in hemodialysis patients.
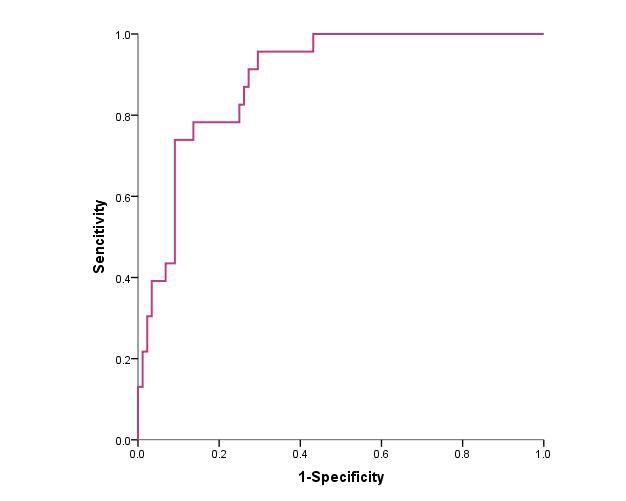
Figure 2: Receiver operator characteristic (ROC) curve analysis of soluble suppression of tumorigenesis-2 (sST2) combined with N-terminal pro-brain natriuretic peptide (BNP) in hemodialysis patients [area under the curve (AUC): 0.892, sensitivity: 0.957, specificity: 0.795].
Discussion
The cardiovascular and renal systems maintain the stability of blood volume, vascular tension, and hemodynamics through two-way interaction. The primary dysfunction of one organ leads to the progressive decline of the two organ systems, known as the cardio-renal system. Chronic kidney-heart disease is characterized by cardiovascular dysfunction based on chronic kidney disease12. Left ventricular hypertrophy (LVH) is very common in MHD patients. LVH occurs in approximately 69 % of pediatric patients and 75 % of adult patients at the commencement of dialysis, and almost 100 % of patients after five years of dialysis13,14. Cardiomyopathy (uremic cardiomyopathy), impaired diastolic filling, myocardial fibrosis, and coronary microvascular disease can also be seen. Vascular changes include atherosclerosis, vascularization, and loss of vascular elasticity. According to the statistics of the United States Renal Data System (USRDS), the mortality caused by CVD in ESRD patients in the United States accounted for 41.6 %, which was significantly higher than the general population and 10-20 x greater than that of the general population. In addition, about 30 % of dialysis patients are hospitalized due to CVD every year15. CVD remains the leading cause of death in ESRD16. HF is one of the most severe complications in dialysis treatment of MHD patients, and it is also a high-risk factor for death. During HF in MHD patients, ventricular remodeling will occur, mainly by increased cardiac load and left ventricular dilation. Therefore, early diagnosis and treatment are particularly important. Due to the atypical symptoms of mild heart failure, it is easy to miss the diagnosis, thus losing the best treatment opportunity and increasing the mortality from cardiovascular diseases in MHD patients17,18. Therefore, exploring effective laboratory indicators to help clinical prediction of HF in MHD patients is significant.
ST2 has two forms: ST2L and sST2. sST2 is a prognostic marker of congestive heart failure14. When stress stimulates cardiomyocytes, IL-33 can bind to ST2L, activating downstream pathways and exerting cardiac protection19. However, sST2 can competitively bind IL-33 and block the entry of IL-33 into the corresponding signaling pathways for cardiac protection, leading to cardiac remodeling and ventricular dysfunction. In the state of cardiac muscle fiber stretching and tension, that is, when human ventricular capacity overload and pressure load increase, as is commonly seen during HF, cardiac myocytes will secrete BNP, so serum NT-proBNP will increase. In this study, MHD patients with HF presented higher age, increased incidence of CHD, LVEDD, PAP, sST2, BNP, and iPTH, and lower EF. In MHD patients with heart failure, the increased myocardial stiffness and diastolic filling pressure result in abnormal left ventricular diastolic function. During the progression of HF, ventricular volume index and ventricular volume increase will further activate the renin-aldosterone-angiotensin system (RAAS) and promote cardiac functional compensation. At the same time, cardiomyocytes inhibit RAAS through massive synthesis and secretion of NT-proBNP20,21. In the present study, logistic regression analysis determined that age, serum sST2, and BNP were independent risk factors of HF in MHD patients. It was also found that PAP was positively correlated with sST2. Therefore, high concentrations of sST2 may predict HF in MHD.
In this study, the ROC curve analysis ascertained that the sensitivity and specificity of sST2 and BNP in predicting HF of MHD patients were 0.783, 0.913 and 0.830, 0.761, respectively, indicating that sST2 and BNP may have certain predictive of the occurrence of HF in MHD. A meta-analysis has previously determined that the AUC of sST2 in heart failure was 0.75, slightly lower than our result22. Moreover, the AUC of sST2 combined with BNP was 0.892, with the sensitivity and specificity being 0.957 and 0.705, respectively. When combining the sST2 and BNP results, the sensitivity is higher, but the cut values are higher than sST2 alone. Thus, the conclusion that combining the two is more valuable was not supported, which may be related to the small sample size, courses, and/or selection bias. However, here for the first time, sST2 is of higher value than BNP in independently predicting HF in MHD patients.
In addition, sST2 was negatively correlated with calcium and inorganic phosphorus in MHD, but no correlation was found between iPTH and sST2. ST2 is associated with parathyroid hormone in CKD patients23. Parathyroid hormone is involved in maintaining mineral balance, and when abnormal, mineral and bone metabolism can be disrupted. IL-33 and ST2 may be regulatory targets of parathyroid hormone24,25. It was determined that 25-OH VitD3 was lower in MHD patients with heart failure, while iPTH did not change between groups, suggesting that iPTH is unrelated to HF in MHD.
In the subgroup analysis of patients with HF26, high sST2 level was a prognostic factor for patients with glomerular filtration rate <60 mL/min/1.73m2. Similarly, higher sST2 concentration has recently been associated with the development of CKD27,28, and the mortality in MHD patients is associated with sST2 levels29. Therefore, elevated sST2 may indicate subclinical cardiovascular disease, directly affect renal function or affect systemic processes in the heart and kidney. The serum sST2 level was higher in CKD patients, and the titer was correlated with the severity of the disease. The cross-sectional design of this study did not establish a healthy control group, excluding the effect of renal function, nor did it analyze the HF or ESRD prognosis of the MHD patients. A follow-up multi-center study would further explore the relationship between sST2 and patient mortality and a set control group of people without diseases. Nevertheless, this study has uncovered for the first time that sST2 can predict HF in MHD patients and may assist in the early diagnosis of HF in MHD patients.
In conclusion, sST2 can be used to predict HF in MHD patients and can assist in the early diagnosis and prevention of HF in MHD patients.
Conflict of interest
Authors report no potential conflict of interest.
Acknowledgement
Xiaowan Zhou and Feng Yi contributed equally to this study; both are the first authors. There is no funding to declare. Written informed consent for the publication of patient data/images was obtained from the patient. The authors would like to express sincere gratitude to our colleagues who contributed to the research while their names do not appear on the paper.
References
- Yasue H, Yoshimura M, Sumida H, Kikuta K, Kugiyama K, Jougasaki M, et al. Localization and mechanism of secretion of B-type natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure. Circulation. 1994; 90: 195-203.
- Januzzi JL Jr, Rehman SU, Mohammed AA, Bhardwaj A, Barajas L, Barajas J, et al. Use of amino-terminal pro-B-type natriuretic peptide to guide outpatient therapy of patients with chronic left ventricular systolic dysfunction. J Am Coll Cardiol. 2011; 58: 1881-1889.
- Januzzi JL, van Kimmenade R, Lainchbury J, Bayes-Genis A, Ordonez-Llanos J, Santalo-Bel M, et al. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: the International Collaborative of NT-proBNP Study. Eur Heart J. 2006; 27: 330-337.
- Aimo A, Vergaro G, Passino C, Ripoli A, Ky B, Miller WL, et al. Prognostic Value of Soluble Suppression of Tumorigenicity-2 in Chronic Heart Failure: A Meta-Analysis. JACC Heart Fail. 2017; 5: 280-286.
- Dong G, Chen H, Zhang H, Gu Y. Long-Term and Short-Term Prognostic Value of Circulating Soluble Suppression of Tumorigenicity-2 Concentration in Chronic Heart Failure: A Systematic Review and Meta-Analysis. Cardiology. 2021; 146: 433-440.
- Bayes-Genis A, Zamora E, de Antonio M, Galán A, Vila J, Urrutia A, et al. Soluble ST2 serum concentration and renal function in heart failure. J Card Fail. 2013; 19: 768-775.
- Choi YB, Lee MJ, Park JT, Han SH, Kang SW, Yoo TH, et al. Prognostic value of soluble ST2 and soluble LR11 on mortality and cardiovascular events in peritoneal dialysis patients. BMC Nephrol. 2020; 21: 228.
- Seo SM, Kim SH, Kim Y, Yoon HE, Shin SJ. Prognostic Utility of Soluble Suppression of Tumorigenicity 2 level as a Predictor of Clinical Outcomes in Incident Hemodialysis Patients. Int J Med Sci. 2018; 15: 730-737.
- Tuegel C, Katz R, Alam M, Bhat Z, Bellovich K, de Boer I, et al. GDF-15, Galectin 3, Soluble ST2, and Risk of Mortality and Cardiovascular Events in CKD. Am J Kidney Dis. 2018; 72: 519-528.
- Zhang Z, Shen B, Cao X, Liu Z, Chen X, Nie Y, et al. Increased Soluble Suppression of Tumorigenicity 2 Level Predicts All-Cause and Cardiovascular Mortality in Maintenance Hemodialysis Patients: A Prospective Cohort Study. Blood Purif. 2017; 43: 37-45.
- Yap J, Lim FY, Gao F, Teo LL, Lam CS, Yeo KK. Correlation of the New York Heart Association Classification and the 6-Minute Walk Distance: A Systematic Review. Clin Cardiol. 2015; 38: 621-628.
- Di Lullo L, Bellasi A, Barbera V, Russo D, Russo L, Di Iorio B, et al. Pathophysiology of the cardio-renal syndromes types 1-5: An uptodate. Indian Heart J. 2017; 69: 255-265.
- Foley RN, Parfrey PS, Kent GM, Harnett JD, Murray DC, Barre PE. Serial change in echocardiographic parameters and cardiac failure in end-stage renal disease. J Am Soc Nephrol. 2000; 11: 912-916.
- Zoccali C, Benedetto FA, Mallamaci F, Tripepi G, Giacone G, Stancanelli B, et al. Left ventricular mass monitoring in the follow-up of dialysis patients: prognostic value of left ventricular hypertrophy progression. Kidney Int. 2004; 65: 1492-1498.
- Krediet RT, Boeschoten EW, Dekker FW. Are the high mortality rates in dialysis patients mainly due to cardiovascular causes? Nephrol Dial Transplant. 2012; 27: 481-483.
- Sowers JR. Diabetes mellitus and vascular disease. Hypertension. 2013; 61: 943-947.
- Lloyd-Jones DM, Goff DC, Stone NJ. Treatment of Blood Cholesterol to Reduce Risk for Atherosclerotic Cardiovascular Disease. Ann Intern Med. 2016; 164: 135-136.
- Drew DA, Weiner DE, Tighiouart H, Scott T, Lou K, Kantor A, et al. Cognitive function and all-cause mortality in maintenance hemodialysis patients. Am J Kidney Dis. 2015; 65: 303-311.
- Sanada S, Hakuno D, Higgins LJ, Schreiter ER, McKenzie AN, Lee RT. IL-33 and ST2 comprise a critical biomechanically induced and cardioprotective signaling system. J Clin Invest. 2007; 117: 1538-1549.
- Oldfield CJ, Duhamel TA, Dhalla NS. Mechanisms for the transition from physiological to pathological cardiac hypertrophy. Can J Physiol Pharmacol. 2020; 98: 74-84.
- Cantor EJ, Babick AP, Vasanji Z, Dhalla NS, Netticadan T. A comparative serial echocardiographic analysis of cardiac structure and function in rats subjected to pressure or volume overload. J Mol Cell Cardiol. 2005; 38: 777-786.
- Yang C, Fan Z, Wu J, Zhang J, Zhang W, Yang J, et al. The Diagnostic Value of Soluble ST2 in Heart Failure: A Meta-Analysis. Front Cardiovasc Med. 2021; 8: 685904.
- Bao YS, Na SP, Zhang P, Jia XB, Liu RC, Yu CY, et al. Characterization of interleukin-33 and soluble ST2 in serum and their association with disease severity in patients with chronic kidney disease. J Clin Immunol. 2012; 32: 587-594.
- Torres VE. Treatment strategies and clinical trial design in ADPKD. Adv Chronic Kidney Dis. 2010; 17: 190-204.
- Zaiss MM, Kurowska-Stolarska M, Böhm C, Gary R, Scholtysek C, Stolarski B, et al. IL-33 shifts the balance from osteoclast to alternatively activated macrophage differentiation and protects from TNF-alpha-mediated bone loss. J Immunol. 2011; 186: 6097-6105.
- Bayes-Genis A, Zamora E, de Antonio M, Galán A, Vila J, Urrutia A, et al. Soluble ST2 serum concentration and renal function in heart failure. J Card Fail. 2013; 19: 768-775.
- Ho JE, Hwang SJ, Wollert KC, Larson MG, Cheng S, Kempf T, et al. Biomarkers of cardiovascular stress and incident chronic kidney disease. Clin Chem. 2013; 59: 1613-1620.
- O’Seaghdha CM, Hwang SJ, Ho JE, Vasan RS, Levy D, Fox CS. Elevated galectin-3 precedes the development of CKD. J Am Soc Nephrol. 2013; 24: 1470-1477.
- Wang S, Wei F, Chen H, Wang Z, Zhang R, Jiang A. The Prognostic Value of Soluble ST2 in Maintenance Hemodialysis Patients: A Meta-Analysis. Blood Purif. 2020; 49: 114-120.