RESEARCH ARTICLE
Hippokratia 2024, 28(4): 158-164
Golnas P1, Golna C1, Kontogiorgos Y2, Christodoulou T2, Konstantopoulou T2, Souliotis K1,3
1Health Policy Institute, Maroussi
2Janssen Hellas, Pefki
3Department of Social and Education Policy, University of Peloponnese, Corinth
Greece
![]()
Abstract
Background: Daratumumab, an anti-cancer monoclonal antibody available in a subcutaneous and intravenous formulation for use in the day hospital setting, is indicated for patients with relapsed or refractory multiple myeloma. This study evaluated the impact of using subcutaneous instead of intravenous formulation in the Greek National Health System.
Methods: We developed a resource optimization tool to calculate the time for each patient and the impact on hospital capacity when using the subcutaneous versus the intravenous formulation of daratumumab. The free time for each patient and the potential additional number of infusions that could be performed in the hospital are estimated by this tool, assuming all freed time is allocated to treating more oncological patients. Sequential calculations were performed, followed by a sensitivity analysis on a range of hospital capacity for oncology infusions (50-250 /day) and intravenous daratumumab patient numbers (10-160) to reflect the reality in Greece.
Results: Subcutaneous use of daratumumab resulted, across all cases, in 60.86-85.94 hours saved per year per intravenous patient and a 7-178 % increase in the hospital’s capacity to provide additional oncology-related infusions. Results were consistent regardless of hospital size and daratumumab patient populations.
Conclusions: Using daratumumab subcutaneously rather than intravenously in eligible patients in the Greek National Health System may reduce patient treatment burden and increase efficiencies, regardless of hospital size. HIPPOKRATIA 2024, 28 (4):158-164.
Keywords: Multiple myeloma, efficiency, Greece, National Health System, subcutaneous, intravenous
Corresponding author: Prof. Kyriakos Souliotis, Department of Social and Education Policy, University of Peloponnese, Corinth, Greece, e-mail: info@ksouliotis.gr
Introduction
In cases where more than one formulation of the same treatment for life-threatening, chronic conditions is available, for instance, intravenous (IV) and subcutaneous (SC), the choice of mode of administration has a critical impact not only on patient quality of life, defined primarily by patient and carer time but also on health system efficiency and treatment outcomes. The former is defined by optimizing resource use and freeing up health care professionals’ time and, thus, system capacity1,2. This is especially true in resource-deprived settings3, where restricted capacity may result in delays in treatment and long waiting times for patients. These may potentially risk suboptimal therapeutic results.
It is especially critical when the two alternative treatment formulations share an effectiveness and safety profile. For example, in relapsed or refractory multiple myeloma (MM), the phase III COLUMBA trial demonstrated noninferiority of the SC formulation of a human monoclonal IgG1κ antibody that acts against the CD38 antigen, daratumumab, when compared to its IV formulation, in terms of efficacy and pharmacokinetics4-7 and an improved safety profile8. In addition, daratumumab SC had significantly shorter administration time than its IV formulation (3-5 minutes vs 3-7 hours, respectively), lower rates of infusion-related reactions (12.7 vs 34.5 %), and lower volume of infusion (median 15 vs 500-1000 ml)4,9-11.
Understanding how to optimize the best use of available alternative formulations of the same treatment amongst eligible patients can inform more efficient management decisions, including cost efficiency. Such exercises might be even more important in healthcare settings, such as Greece, where, following the financial crisis of 2009, spending on healthcare as a percentage of the Gross Domestic Product has remained lower than the European Union (EU27) average (in 2022, 8.5 vs 10.4 %)12 and hospitals are grappling with cost containment13. This is further exacerbated by the reimbursement structure of care provision in the Greek National Health System (NHS), which is funded by a dual system of social insurance reimbursement for service provision and State subsidies from general taxation14. Mainly as regards reimbursement of daycare for the administration of treatment in life-threatening, chronic conditions, an official rate of €80 per IV infusion (day hospital care) has been set for NHS hospitals15, to be paid by the third party-payer, namely the National Organization for the Provision of Healthcare Services (EOPPY). This rate is assumed to reflect hospital costs for drug and patient preparation, drug administration (chair time), and management of any required patient support. On the contrary, SC administration is assumed to cost €0, as EOPYY does not explicitly stipulate a reimbursable fee for SC administration.
In any case, persistent hospital understaffing coupled with the increase in the prevalence and incidence of non-communicable diseases, primarily cancer, has added to the capacity challenges faced by the Greek NHS. Further, delays in clearing payments and annual state subsidies of both human resource and capital investment costs have skewed the potential of Greek NHS hospitals to increase their “real” revenue through more efficient use of available resources16.
Therefore, a defined need exists to model and estimate the true impact of decisions to use alternative formulations of the same treatment on hospital capacity to treat patients, patient time, and, eventually, hospital revenues. This study aims to assess the impact of daratumumab SC vs IV administration in eligible patients in the Greek NHS in case studies that reflect potential combinations of demand and supply circumstances in public hospital day clinics.
Material and Methods
We developed a resource optimization tool in Microsoft Excel to calculate the impact on day hospital capacity in the Greek NHS and the time saved using SC instead of IV daratumumab for each patient. The tool estimates the free time per individual patient and the potential additional number of infusions that could be performed in the hospital using SC instead of IV daratumumab, assuming all time retrievals associated with the briefer chair time administering SC daratumumab are reallocated to treating either more oncological patients in general or more MM patients specifically with SC daratumumab. The time required per oncology-related infusion is calculated based on the total number of oncology-related infusions (infusions/day) and hospital working hours. In the scenario before the use of SC daratumumab, patients who were newly eligible for daratumumab-based treatment received IV daratumumab; in the scenario after the use of SC daratumumab, patients who were newly eligible for daratumumab-based treatment received SC daratumumab. The analysis does not consider a switch from IV to SC daratumumab for patients that have already initiated a daratumumab-based treatment. Daycare cost for IV treatments is set at the official rate of €80 per IV infusion, as reimbursed by the third-party payer (EOPYY).
The analysis focuses on one daratumumab-based regimen/population at a time, and more specifically:
- Newly diagnosed multiple myeloma (NDMM) patients ineligible for autologous stem cell transplant (ASCT) administered with daratumumab, lenalidomide, and dexamethasone (DRd).
- NDMM patients ineligible for ASCT administered with daratumumab, bortezomib, melphalan, and prednisolone (DVMP).
- NDMM eligible for ASCT administered with daratumumab, bortezomib, thalidomide, and prednisolone (DVTd).
- MM patients from the second line administered with DRd.
- MM patients from the second line administered with daratumumab, bortezomib, and dexamethasone (DVd).
- MM patients from the third line administered with daratumumab monotherapy.
Infusion/injection times and non-infusion/injection patient chair times for daratumumab are as reported in the daratumumab time and motion study (TMS)17, and day hospital visits are derived from daratumumab dosing schedules in the summary of product characteristics18. Base non-infusion/injection patient chair times for IV and SC daratumumab regimens are added to the infusion/injection times to derive total chair time. Chair time retrievals have been converted to additional oncology infusions and multiplied by the officially reimbursed rate per infusion in daycare to calculate potential additional income for the hospital, assuming available resources (infrastructure and human) are sufficient to meet this increased infusion volume.
As published data regarding active oncology patients from each Greek hospital is missing, sequential calculations were performed, followed by a sensitivity analysis on oncology-related infusion capacity and IV daratumumab patient numbers. We chose different sets of oncology/IV daratumumab patients to reflect the most probable size of oncology hospital establishments in Greece:
- Hospital with 50 infusions/day and 10 IV daratumumab patients.
- Hospital with 70 infusions/day and 20 IV daratumumab patients.
- Hospital with 110 infusions/day and 40 IV daratumumab patients.
- Hospital with 150 infusions/day and 80 IV daratumumab patients.
- Hospital with 200 infusions/day and 120 IV daratumumab patients.
- Hospital with 250 infusions/day and 160 IV daratumumab patients.
All the above sets were tested in a follow-up sensitivity analysis – lower and upper bounds were calculated as ±10 % of the base case value.
Results
Regardless of hospital size and daratumumab patient populations, across all analyses performed, SC daratumumab administration is anticipated to result in significant time retrievals in hours per year and per IV patient and in measurable increases in hospitals’ capability to treat general oncology patients. More specifically, in the first case study of a hospital with a capacity of 50 infusions/day and with 10 patients on daratumumab IV (± 10 % of patients on IV daratumumab), using the SC formulation would free time for up to 28 additional oncology related infusions/week (Figure 1). If an €80 reimbursement rate per day care infusion is applied15, chair time savings may translate into an additional revenue of up to €1,920 per week for the hospital.

Figure 1: Case study one concerning hospitals with 50 infusions/day and 10 intravenous daratumumab patients (±10 %).
*: Includes induction and consolidation only, ASCT: autologous stem cell transplant, Dara: daratumumab, DRd: daratumumab/lenalidomide/dexamethasone, DVd: daratumumab/bortezomib/dexamethasone, DVTd: daratumumab/bortezomib/thalidomide/dexamethasone, MM: multiple myeloma, IV: intravenous, DVMP: daratumumab/bortezomib/melphalan/prednisolone, NDMM: newly diagnosed multiple myeloma.
In the second case study of a hospital with a capacity of 70 infusions/day and with 20 patients on IV daratumumab (± 10 % of patients on daratumumab IV), using the SC formulation would free time for up to 69 additional oncology-related infusions/week (Figure 2). Applying the daily reimbursement rate used in case study 1 would potentially result in additional revenue of up to €4,960 per week for the hospital. In the third case study of a hospital with 110 infusions/day capacity and 40 patients on IV daratumumab (±10 %), the SC formulation would free time for up to 215 additional oncology related infusions/week (Figure 3). Applying the daily reimbursement rate used in case study 1 would potentially result in additional revenue of up to €16,080 per week for the hospital.

Figure 2: Case study two concerning hospitals with 70 infusions/day and 20 intravenous daratumumab patients (±10 %).
*: Includes induction and consolidation only, ASCT: autologous stem cell transplant, Dara: daratumumab, DRd: daratumumab/lenalidomide/dexamethasone, DVd: daratumumab/bortezomib/dexamethasone, DVTd: daratumumab/bortezomib/thalidomide/dexamethasone, MM: multiple myeloma, IV: intravenous, DVMP: daratumumab/bortezomib/melphalan/prednisolone, NDMM: newly diagnosed multiple myeloma.
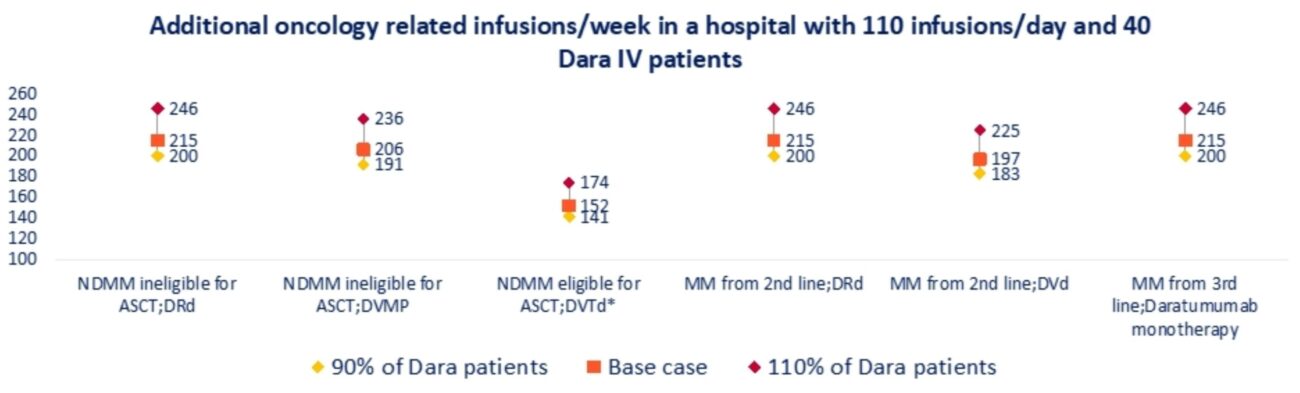
Figure 3: Case study three concerning hospitals with 110 infusions/day and 40 intravenous daratumumab patients (±10 %).
*: Includes induction and consolidation only, ASCT: autologous stem cell transplant, Dara: daratumumab, DRd: daratumumab/lenalidomide/dexamethasone, DVd: daratumumab/bortezomib/dexamethasone, DVTd: daratumumab/bortezomib/thalidomide/dexamethasone, MM: multiple myeloma, IV: intravenous, DVMP: daratumumab/bortezomib/melphalan/prednisolone, NDMM: newly diagnosed multiple myeloma
Further, in a hospital with 150 infusions/day and 80 patients on IV daratumumab (±10 %), using the SC formulation would free time for up to 580 additional oncology related infusions/week and contribute to a potential additional revenue for the hospital of €44,160 per week (Figure 4).
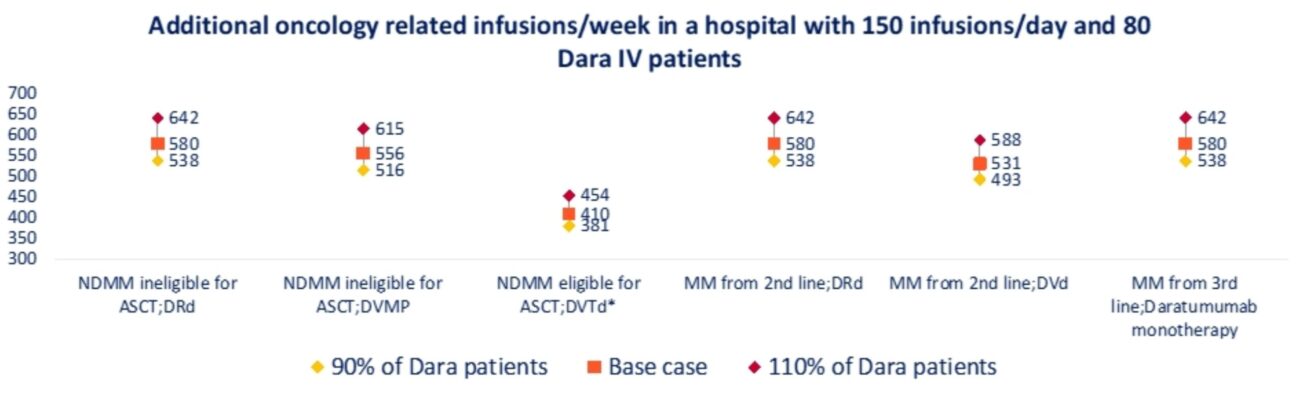
Figure 4: Case study four concerning hospitals with 150 infusions/day and 80 intravenous daratumumab patients (±10 %).
*: Includes induction and consolidation only, ASCT: autologous stem cell transplant, Dara: daratumumab, DRd: daratumumab/lenalidomide/dexamethasone, DVd: daratumumab/bortezomib/dexamethasone, DVTd: daratumumab/bortezomib/thalidomide/dexamethasone, MM: multiple myeloma, IV: intravenous, DVMP: daratumumab/bortezomib/melphalan/prednisolone, NDMM: newly diagnosed multiple myeloma
Results are consistent in yet larger hospitals with more patients on IV daratumumab. For instance, in a hospital with a capacity of 200 infusions/day and with 120 patients on IV daratumumab (±10 %) and in a hospital with a capacity of 250 infusions/day and with 160 patients on IV daratumumab (±10 %), using the SC formulation would free time for up to 1,154 and 1,918 additional oncology related infusions/week, respectively and contribute to a potential additional revenue of €88,960 and €148,960 per week for the hospital (Figure 5 and Figure 6).

Figure 5: Case study five concerning hospitals with 200 infusions/day and 120 intravenous daratumumab patients (±10 %).
*: Includes induction and consolidation only, ASCT: autologous stem cell transplant, Dara: daratumumab, DRd: daratumumab/lenalidomide/dexamethasone, DVd: daratumumab/bortezomib/dexamethasone, DVTd: daratumumab/bortezomib/thalidomide/dexamethasone, MM: multiple myeloma, IV: intravenous, DVMP: daratumumab/bortezomib/melphalan/prednisolone, NDMM: newly diagnosed multiple myeloma
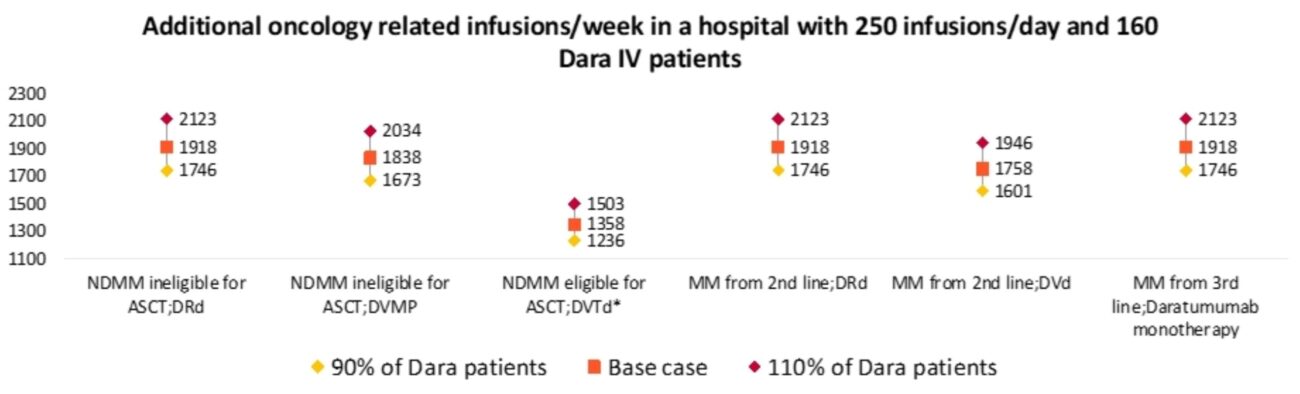
Figure 6: Case study six concerning hospitals with 250 infusions/day and 160 intravenous daratumumab patients (±10 %).
*: Includes induction and consolidation only, ASCT: autologous stem cell transplant, Dara: daratumumab, DRd: daratumumab/lenalidomide/dexamethasone, DVd: daratumumab/bortezomib/dexamethasone, DVTd: daratumumab/bortezomib/thalidomide/dexamethasone, MM: multiple myeloma, IV: intravenous, DVMP: daratumumab/bortezomib/melphalan/prednisolone, NDMM: newly diagnosed multiple myeloma
The case studies modeled above are summarized in Table 1 below. Our analysis also confirmed that using SC instead of IV daratumumab would free up to 86 hours per patient per year, thus substantially reducing the treatment burden for patients and carers/families. Table 2 depicts the difference between SC and IV formulation regarding patient time per year, while Table 3 depicts patient time per patient sub-population gains.
Discussion
This analysis aimed to model the impact on hospital efficiencies and patient time of using SC instead of IV daratumumab in eligible patients in the Greek NHS (day hospitals). Our analysis confirms that using SC as an alternative to IV daratumumab in a day hospital in the Greek NHS would result in reduced patient treatment burden and increased healthcare efficiencies, independent of the size of the hospital establishment. This may also translate into additional revenue for the hospital if the NHS moves towards greater financial independence of its hospitals from State subsidies19.
Our findings support earlier findings20 on the potential impact of using SC instead of IV daratumumab, which confirmed that in resource-stretched settings, SC daratumumab might support centers in meeting patient demand without the need to increase their actual capacity. Our analysis is based on the daratumumab TMS17, which concluded that SC daratumumab reduces median total health care professionals (HCPs) time by 63.8 and 49.5 %, respectively, for first and subsequent treatments. Over the total anticipated treatments per year, the study calculated an estimated reduction in HCP time of 50 % in years 1 and 2 and an estimated reduction in chair time of 97 % for first and subsequent treatments. Savings were derived primarily from reduced drug preparation and administration/care times. Real-world findings confirmed these chair time savings21 and revealed that, over 18 months, the use of SC daratumumab formulation resulted in a potential 1,785 hours of infusion chair time savings when compared to the use of IV formulation.
These results agree with findings from other therapeutic areas where SC formulations have been compared with their IV counterparts. In non-Hodgkin’s lymphoma and breast cancer, significant savings in terms of lower patient preparation time were estimated when using SC instead of IV formulations of the same therapies (rituximab and trastuzumab, respectively) across 17 hospitals in Italy. Total time differences were 3.3 hours per treatment in hematology and for the first cycle in early breast cancer or 23.55 hours for an entire course of treatment per patient in hematology and 17.2 hours for patient preparation in oncology22. In Spain, the transition from IV to SC trastuzumab led to a 50 % reduction in active HCP time, primarily from the redundancy of the need to install and remove IV catheters, line flushing, and drug reconstitution. Overall, SC administration led to fivefold reductions in patient chair time and room time23. In the USA, amongst non-Hodgkin’s lymphoma patients, the transition of 20 % of patients from IV to SC rituximab was estimated to increase provider capacity by 270 hours and free 470 hours of patient time, in the cohort modelled24. Other analyses for infliximab in rheumatoid arthritis and inflammatory bowel disease revealed lower administration costs in the subcutaneous related to intravenous routes, and additional indirect benefits, such as less pressure on infusion unit waiting times, greater protection during infectious diseases outbreaks, such as COVID-19, and reduced patient “out-of-pocket” costs25.
Further, patient satisfaction with treatment increases when SC are used instead of IV formulations. For SC daratumumab in particular, Usmani et al5 surveyed MM patients for their satisfaction with treatment. They concluded that a numerically more significant proportion of patients in the SC group expressed positive perceptions of therapy for most questions. A previous study on bortezomib in MM26 also showed patient preference for the SC compared to the IV formulation – this may also be related to the 38 % reduction in chair time and 27 % reduction in infusion center visit time associated with the SC formulation. In early human epidermal growth factor receptor 2 (HER-2) positive cancer, more than 85 % of patients preferred SC administration of trastuzumab over IV administration, mainly because it was timesaving27. The SC combination of trastuzumab with pertuzumab for HER-2 positive cancer was also preferred by 85 % of patients in the phase II clinical trial over IV pertuzumab plus trastuzumab28. In diffuse large B-cell lymphoma, patients on SC rituximab plus chemotherapy reported higher scores for “impact on activities of daily living”, “convenience” and “satisfaction” versus patients in IV rituximab plus chemotherapy29. In rheumatoid arthritis, a recent survey of patient preferences for treatment mode of biologics in Japan30 revealed a preference for in-hospital injection (18 %) versus in-hospital infusion (15.3 %). Self-injection was the most preferred route of administration (66.8 %)30.
Our study is limited by the lack of officially published indicators, such as hospital capacity for daycare, number of patients treated in daycare, opening hours, etc., which would allow for a more accurate representation of the specific study inputs. This limitation is addressed through the testing of five different, hypothetical case studies with varied combinations of hospital capacity and patients on treatment, each including sensitivity analysis, to test the robustness of our results and allow for probable combinations in real-life Greek NHS. Additionally, as the perspective of the economic analysis is that of the third-party payer, all calculations use only officially reimbursed rates, which may not reflect actual resource use cost for some services in the NHS hospitals. In the future, it would be critical to complement this model with a wider analysis of cost implications, including all hospital and third-party costs, to further inform hospital decision-making processes on allocating scarce resources.
Conclusion
Our study confirmed that the use of SC compared to IV daratumumab in eligible patients with relapsed or refractory MM in the Greek NHS has the potential to free up scarce resources, increase capacity to treat, and reduce patient and carer time, thus improving overall efficiency and patient experience with the health system.
Conflict of interest
This study was funded by Janssen Hellas. TC, IK, TK are employees of Janssen.
Acknowledgement
A part of this work was previously presented at the ISPOR Europe 2023 Conference (Copenhagen, Denmark) and its abstract EE531 was published in Value in Health. 2023; 26 Supplement: S154.
References
- Drill E, Qiu A, Shapouri S, To TM, Ravelo A, Schade J, et al. Real-World Assessment of Patient Care and Practice Efficiency With the Introduction of Subcutaneous Rituximab. Oncology (Williston Park). 2021; 35: 804-811.
- North RT, Harvey VJ, Cox LC, Ryan SN. Medical resource utilization for administration of trastuzumab in a New Zealand oncology outpatient setting: a time and motion study. Clinicoecon Outcomes Res. 2015; 7: 423-430.
- Olivera Changra H, Robles Díaz JF. Costos de la administración intravenosa vs. subcutánea del trastuzumab en pacientes peruanas con cáncer de mama HER2 positivo. Un análisis observacional de los costos directos e indirectos [Costs of intravenous vs. subcutaneous administration of trastuzumab in peruvian patients with HER2-positive breast cancer – An observational analysis of direct and indirect costs]. J Healthc Qual Res. 2022; 37: 147-154.
- Usmani SZ, Nahi H, Legiec W, Grosicki S, Vorobyev V, Spicka I, et al. Final analysis of the phase III non-inferiority COLUMBA study of subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma. Haematologica. 2022; 107: 2408-2417.
- Usmani SZ, Mateos MV, Hungria V, Iida S, Bahlis NJ, Nahi H, et al. Greater treatment satisfaction in patients receiving daratumumab subcutaneous vs. intravenous for relapsed or refractory multiple myeloma: COLUMBA clinical trial results. J Cancer Res Clin Oncol. 2021; 147: 619-631.
- Shibayama H, Matsumoto M, Kosugi H, Shibayama K, Yamazaki H, Iida S. Subcutaneous delivery of daratumumab in Japanese patients with relapsed/refractory multiple myeloma. Int J Hematol. 2021; 113: 112-121.
- San-Miguel J, Usmani SZ, Mateos MV, van de Donk NWCJ, Kaufman JL, Moreau P, et al. Subcutaneous daratumumab in patients with relapsed or refractory multiple myeloma: Part 2 of the open-label, multicenter, dose-escalation phase 1b study (PAVO). Haematologica. 2021; 106: 1725-1732.
- Mateos MV, Cavo M, Blade J, Dimopoulos MA, Suzuki K, Jakubowiak A, et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet. 2020; 395: 132-141.
- Sanchez L, Richter J, Cho HJ, Jagannath S, Madduri D, Parekh S, et al. Subcutaneous daratumumab and hyaluronidase-fihj in newly diagnosed or relapsed/refractory multiple myeloma. Ther Adv Hematol. 2021; 12: 2040620720987075.
- Chari A, San-Miguel J, McCarthy H, Suzuki K, Hungria VTM, Sureda A, et al. Subcutaneous Daratumumab Plus Standard Treatment Regimens in Patients with Multiple Myeloma across Lines of Therapy: Pleiades Study Update. Blood. 2019; 134: 3152.
- Paul B, Hamadeh I, Atrash S, Bhutani M, Voorhees P, Usmani SZ. Daratumumab subcutaneous formulation for the treatment of multiple myeloma. Expert Opin Biol Ther. 2020; 20: 1253-1259.
- OECD/European Commission (2024). Health at a Glance: Europe 2024: State of Health in the EU Cycle. Available at: https://doi.org/10.1787/b3704e14-en, date accessed: 30/9/2024.
- Letsios A, Polyzos N, Poulopoulos C, Skamnakis C. Hospital managers’ participation in operational planning: insights from a recent study in the Greek National Health System. Hippokratia. 2022; 26: 91-97.
- Souliotis K. Facing the impact of persistent economic crisis on healthcare in Greece: The need for a new financing paradigm. Saridi M, Souliotis K (Editors). The Impact and Implications of Crisis: A Comprehensive Approach Combining Elements of Health and Society. Nova Science Publishers, New York, 2018, 293-301.
- Government Gazette Issue (FEK) of the Hellenic Republic. FEK B 2150/2011/27-09-2011: Closed Unified Hospitals and Day Hospital in the National Health Service. Available at: https://search.et.gr/el/fek/?fekId=438293, date accessed: 30/9/2024.
- Kaitelidou D, Katharaki M, Kalogeropoulou M, Economou C, Siskou O, Souliotis K, et al. The impact of economic crisis to hospital sector and the efficiency of Greek public hospitals. EJBSS. 2016; 4: 111-125.
- Slavcev M, Spinelli A, Absalon E, Masterson T, Heuck C, Lam A, et al. Results of a Time and Motion Survey Regarding Subcutaneous versus Intravenous Administration of Daratumumab in Patients with Relapsed or Refractory Multiple Myeloma. Clinicoecon Outcomes Res. 2021; 13: 465-473.
- DARZALEX. ANNEX I. Summary of Product Characteristics. Available at: https://www.ema.europa.eu/en/documents/product-information/darzalex-epar-product-information_en.pdf, date accessed: 30/9/2024.
- Kanavos P, Souliotis K. Reforming health care in Greece: balancing fiscal adjustment with health care needs. Meghir C, Pissarides C, Vayanos D, Vettas N, (Editors). Beyond Austerity: reforming the Greek Economy. MIT Press, Cambridge, Massachusetts, 2017, 359-401.
- Federici C, Rognoni C, Costa F, Armeni P, Crovato E, Bellucci S. Use of Resource Modeling to Quantify the Organizational Impact of Subcutaneous Formulations for the Treatment of Oncologic Patients: The Case of Daratumumab in Multiple Myeloma. Clin Ther. 2022; 44: 1480-1493.
- Davis JA, Youngberg H, Gaffney K, Duco M, Hashmi H. ‘Fast but not so Furious’: Short observation time after subcutaneous Daratumumab administration is both a safe and cost-effective strategy. Clin Lymphoma Myeloma Leuk. 2022; 22: e680-e684.
- Ponzetti C, Canciani M, Farina M, Era S, Walzer S. Potential resource and cost saving analysis of subcutaneous versus intravenous administration for rituximab in non-Hodgkin’s lymphoma and for trastuzumab in breast cancer in 17 Italian hospitals based on a systematic survey. Clinicoecon Outcomes Res. 2016; 8: 227-233.
- Lopez-Vivanco G, Salvador J, Diez R, López D, De Salas-Cansado M, Navarro B, et al. Cost minimization analysis of treatment with intravenous or subcutaneous trastuzumab in patients with HER2-positive breast cancer in Spain. Clin Transl Oncol. 2017; 19: 1454-1461.
- Harvey MJ, Zhong Y, Morris E, Beverage JN, Epstein RS, Chawla AJ. Assessing the transition from intravenous to subcutaneous delivery of rituximab: Benefits for payers, health care professionals, and patients with lymphoma. PLoS One. 2022; 17: e0261336.
- Heald A, Bramham-Jones S, Davies M. Comparing cost of intravenous infusion and subcutaneous biologics in COVID-19 pandemic care pathways for rheumatoid arthritis and inflammatory bowel disease: A brief UK stakeholder survey. Int J Clin Pract. 2021; 75: e14341.
- Barbee MS, Harvey RD, Lonial S, Kaufman JL, Wilson NM, McKibbin T, et al. Subcutaneous versus intravenous bortezomib: efficiency practice variables and patient preferences. Ann Pharmacother. 2013; 47: 1136-1142.
- Sanford M. Subcutaneous trastuzumab: a review of its use in HER2-positive breast cancer. Target Oncol. 2014; 9: 85-94.
- DuMond B, Patel V, Gross A, Fung A, Weber S. Fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection in patients with HER2-positive breast cancer: A multidisciplinary approach. J Oncol Pharm Pract. 2021; 27: 1214-1221.
- Lugtenburg P, Avivi I, Berenschot H, Ilhan O, Marolleau JP, Nagler A, et al. Efficacy and safety of subcutaneous and intravenous rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone in first-line diffuse large B-cell lymphoma: the randomized MabEase study. Haematologica. 2017; 102: 1913-1922.
- Kishimoto M, Yamairi F, Sato N, Kobayashi J, Yamauchi S, Iwasaki T. Patient Preference for Treatment Mode of Biologics in Rheumatoid Arthritis: A 2020 Web-based Survey in Japan. Rheumatol Ther. 2021; 8: 1095-1111.