RESEARCH ARTICLE
Hippokratia 2024, 28(2): 50-55
Yang N1, Fan Y2, Lian Y1
1Department of Gastrointestinal Surgery, Xingtai Central Hospital
2Department of Ophthalmology, Hebei Eye Hospital
Xingtai, Hebei Province, China
![]()
Abstract
Objective: This study aims to assess the feasibility and short-term efficacy of employing laparoscopic surgery for the treatment of right-sided colon cancer complicated by acute intestinal obstruction following intestinal decompression.
Methods: We undertook a retrospective analysis of a cohort of 22 patients (designated as the study group) hospitalized between January 2017 and December 2022 who presented with right-sided colon cancer complicated by acute intestinal obstruction and underwent laparoscopic-assisted right hemicolectomy subsequently to intestinal decompression. The control group consisted of 36 patients who underwent laparoscopic right hemicolectomy for right-sided colon cancer without intestinal obstruction during the same period. We compared the study group and a control group regarding operative time, surgical blood loss, number of lymph nodes harvested, time to first flatus, postoperative hospital stay, and postoperative complications between the two groups.
Results: The operative time for the study group and control group was (181.82 ± 14.84) minutes and (155.75 ± 17.86) minutes, respectively, and the difference was statistically significant (p <0.001). However, we found no significant differences between the two groups in terms of surgical blood loss (89.32 ± 47.62 vs 94.58 ± 42.65) ml), the number of lymph nodes (23.05 ± 5.08 vs 23.50 ± 5.57), time to first flatus (4.36 ± 1.01 vs 3.93 ± 1.09 days), postoperative hospital stay(16.36 ± 3.26 vs 16.17 ± 2.54 days), and incidence of short-term postoperative complications (13.64 % vs 7.69 %).
Conclusion: In individuals diagnosed with right-sided colon cancer and acute intestinal obstruction, the implementation of laparoscopic-assisted right hemicolectomy subsequent to intestinal decompression proves to be a minimally invasive, safe, feasible, and effective intervention. HIPPOKRATIA 2024, 28 (2):50-55.
Keywords: Colon cancer, colectomy, intestinal decompression, intestinal obstruction, laparoscopic surgery
Corresponding author: Yanjun Lian, Department of Gastrointestinal Surgery, Xingtai Central Hospital, No.108 of Steel North Road, Xindu District, Xingtai, Hebei province, 054000, China, tel.: +8603192123376, e-mail: lianalian@163.com
Introduction
Colon cancer is a common malignancy affecting the gastrointestinal tract, with incidence rates falling short only to stomach and esophageal malignancies1 and associated with an extremely high mortality rate2. Based on available data, the annual mortality rate associated with colon cancer is estimated to be around 900,000 individuals, accounting for approximately 10 % of the total number of cancer-induced fatalities3. Colon cancer is commonly classified based on the primary tumor site, with typical classifications into left-sided colon cancer and right-sided colon cancer4. While the clinical treatment of colon cancer typically does not differentiate based on the location of the primary lesion, it is essential to acknowledge that right-sided colon cancer often presents distinct clinical and biological characteristics5. For instance, right-sided colon cancer is more likely to present with tumor rupture, bleeding, and cachexia, while left-sided colon cancer commonly leads to intestinal obstruction6.
Laparoscopic surgery for colon cancer has advantages such as minimal invasiveness, less postoperative pain, quicker recovery of gastrointestinal functions, and shorter hospital stays7. Furthermore, its long-term efficacy has been demonstrated to be comparable to that of open surgery8. However, some patients diagnosed with advanced-stage colon cancer present with acute intestinal obstruction, preventing standard preoperative preparation and necessitating emergency surgery. To perform laparoscopic surgery is challenging in this clinical condition and often hindered by the presence of bowel distention, which results in a reduction of available space within the abdominal cavity9. This emergency approach results in greater surgical trauma, slower recovery, and, due to larger incisions, there is an increased risk of wound infection and delayed healing. These factors subsequently impact later comprehensive therapies.
Right-sided colon cancer has a lower incidence of intestinal obstruction compared to left-sided colon cancer10. The embryonic origins between left-sided and right-sided colon cancers are different11. The BRAF and KRAS gene mutations are more common in right-sided colon cancer, while APC gene mutations are more prevalent in left-sided colon cancer12. In terms of prognosis, patients with right-sided colon cancer generally have a higher mortality rate, whereas left-sided patients typically have better overall survival rates13. In terms of recurrence-free survival, left-sided colon cancer also shows better survival compared to right-sided. Additionally, ileocolonic anastomosis is often required for right-sided colon cancer, while colocolonic anastomosis is mostly needed for left-sided colon cancer14. However, a limited number of prior studies have investigated and presented a comprehensive overview of therapeutic approaches for right-sided colon cancer accompanied by intestinal obstruction, resulting in limited clinical experience.
In this study, we aimed to investigate surgical treatment methods for right-sided colon cancer in conjunction with intestinal obstruction. The study group consisted of patients with right-sided colon cancer complicated by intestinal obstruction who underwent laparoscopic radical right hemicolectomy after decompression. The control group included patients with right-sided colon cancer without intestinal obstruction who met the indications for laparoscopic right hemicolectomy. By conducting a non-inferiority comparison between the study group and the control group, the study demonstrated that laparoscopic surgery after decompression is safe and feasible for patients with right-sided colon cancer complicated by bowel obstruction.
Material and Methods
General data
A total of 22 patients diagnosed with right-sided colon cancer complicated with intestinal obstruction, treated at our hospital between January 2017 and December 2022, were enrolled in the study group. The study group consisted of 10 males and 12 females, aged between 52 and 83 years. The distribution of the tumor locations was four tumors in the hepatic flexure of the colon, eight tumors in the ascending colon, and 10 tumors in the ileocecal region. Tumor locations were confirmed preoperatively by abdominal contrast-enhanced computed tomography (CT) scans (Figure 1) and postoperatively by pathological analysis. None of the patients had detectable distant metastasis. Upon admission, routine procedures such as fasting, gastrointestinal decompression, anti-infection therapy, and fluid resuscitation treatment, along with preoperative bowel cleansing enemas, were administered. During the same period, 36 patients diagnosed with right-sided colon cancer without intestinal obstruction, treated at the hospital, were included in the control group. The cohort consisted of 19 males and 17 females, aged between 48 and 85 years. The distribution of the tumor locations was 12 in the hepatic flexure of the colon, 14 in the ascending colon, and 10 in the ileocecal area, all confirmed by preoperative colonoscopy. Thoracoabdominal contrast-enhanced CT scans were used to exclude distant organ metastasis. Both groups of patients had no underlying diseases that were contraindications for laparoscopic surgery. This study was conducted in accordance with the declaration of Helsinki, following approval of the study protocol by the Ethics Committee of Xingtai Central Hospital (Medical Ethics Committee of the Third Hospital of Xingtai, date: 11/10/2023), and written informed consent was obtained from all participants.
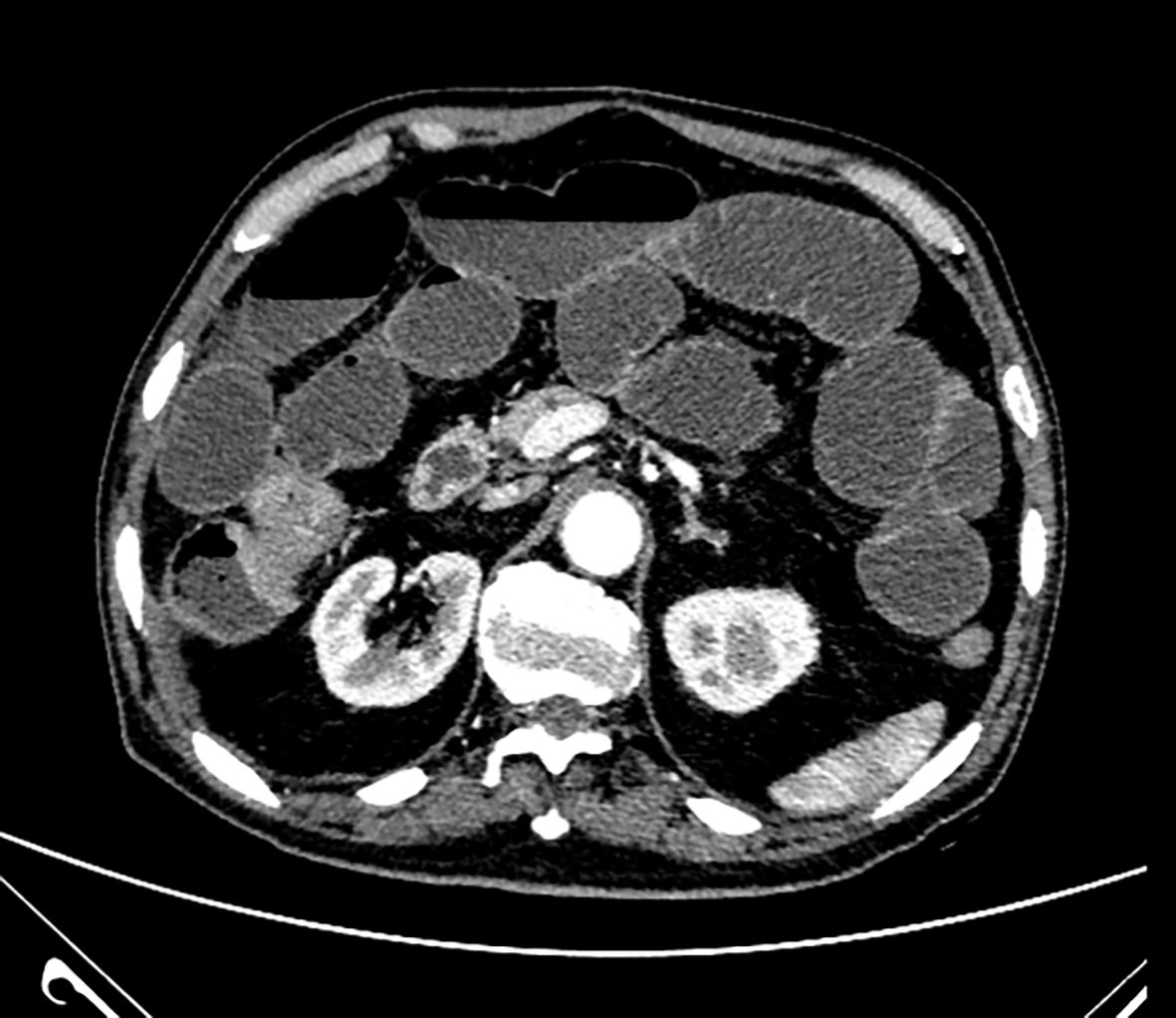
Figure 1: Preoperative axial abdominal contrast-enhanced computed tomography scan showing the cancer located in right-sided colon.
Surgical procedure
Both groups of patients were positioned in a supine lithotomy position and were administered general anesthesia through endotracheal intubation. In the study group, a longitudinal auxiliary incision of approximately five to seven cm was made above the umbilicus. After gaining access to the abdomen cavity, a laparoscopic port was used to safeguard the incision, and the dilated small intestine was extricated through the incision. A 20 cm long section of the ileum near the ileocecal junction was incised along the margin of the mesentery. This procedure was carried out to alleviate the pressure within the small intestine, facilitating decompression and a subsequent reduction in size. If there was also dilation of the ascending colon, a suction device was inserted through the ileal incision and passed through the ileocecal valve into the ascending colon for decompression. After decompression, the incision site in the ileum was sutured using a 3-0 thread, and the small intestine was carefully repositioned into the abdominal cavity. The incision was then closed, with a rubber glove placed over the port (Figure 2). Subsequently, CO2 pneumoperitoneum was established at 12 to 15 mmHg pressure. A trocar with a diameter of 10 mm was inserted approximately three to five cm below the umbilicus for observation. Another trocar with a diameter of 12 mm was inserted below the left costal margin at the midclavicular line. Additionally, a trocar with a diameter of five mm was inserted medial to the left anterior superior iliac spine at the level of the midclavicular line, and two more trocars with a diameter of five mm were inserted at corresponding points on the right side. The surgeons positioned themselves on the patient’s left side, accompanied by an assistant on the right and a camera assistant between the patient’s legs. Upon the conclusion of the laparoscopic surgical procedure, the rubber glove covering the port was removed. Subsequently, extracorporeal tumor resection and anastomosis were performed, and the abdominal incision was sutured. The arrangement of abdominal trocars, maintenance of pneumoperitoneum pressure, and the positioning of the surgeon for the control group were in accordance with the previously mentioned details. Following the laparoscopic mobilization of the intestines, a comparable small incision in the upper abdomen was created, akin to the approach used in the study group. This incision facilitated the extracorporeal resection of the tumor and the establishment of a primary anastomosis.

Figure 2: Post-decompression intraoperative image showing the extricated small intestine through the upper abdominal small incision and the incision being sutured.
A conventional midline approach was applied in both groups. The superior mesenteric vessels and their spaces were identified based on their visual appearance. The procedure involved opening the posterior peritoneum on the left side of the surface of the superior mesenteric vein (SMV) from below, exposing the vessels and closely following the right side of the main trunk of the SMV to ligate and divide the ileocolic artery and vein (Figure 3). The adipose tissue surrounding the lymphatic vessels was excised, and the dissection progressed cranially to mobilize Henle’s trunk and its branches. The (accessory) right colic vein was ligated and severed at its origin. It was subsequently followed by the mobilization of the middle colic artery and vein, with the division of their branches on the right side (Figure 4). The mesenteric space was expanded cranially and to the right side along the Toldt’s space, with care taken to protect the duodenum and pancreas posteriorly. Subsequently, the central part of the gastrocolic ligament was incised to gain access to the smaller sac. In cases where the tumor was situated at the hepatic flexure, the standard protocol involved the dissection of group 6 lymph nodes. Subsequently, these lymph nodes were submitted for postoperative pathological evaluation. The hepatocolic ligament was then incised on the right side, and the ascending colon and ileocecal area were mobilized caudally along the white line of Toldt. This maneuver facilitated the connection of the structures above with the intramesenteric space located on the medial aspect of the ileum. The terminal ileum was mobilized for approximately 10 to 20 cm, concluding the mobilization process.
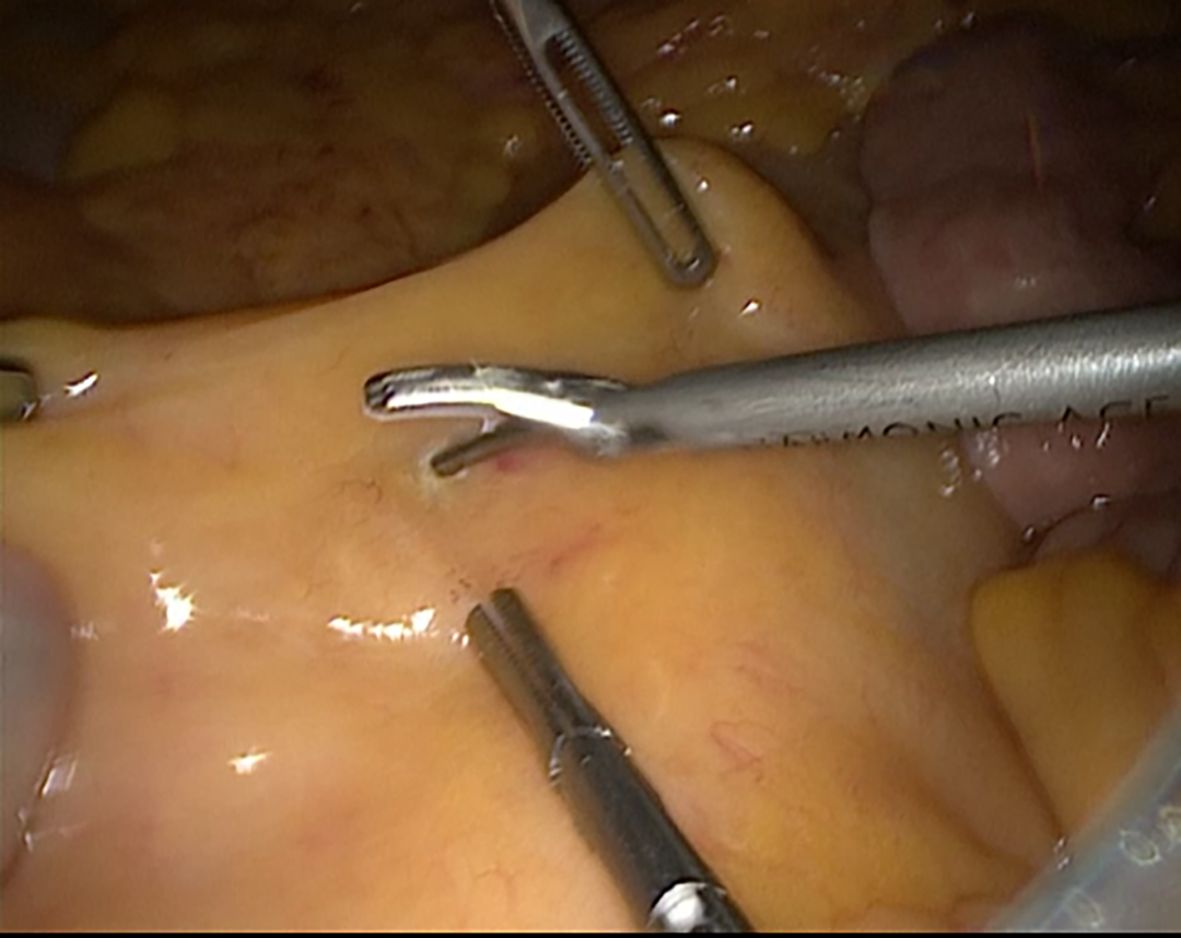
Figure 3: Midline approach for freeing the ileocolic artery and vein.

Figure 4: Intraoperative image following completion of laparoscopic right hemicolectomy, demonstrating the superior mesenteric artery, vein, and their branches post-intervention.
Observational Indicators
A comparative analysis of the general data regarding operative time, intraoperative blood loss, number of lymph nodes harvested, time to first flatus, and postoperative hospital stay between the two groups was conducted. Additionally, an assessment of the incidence of early postoperative abdominal complications (anastomotic leakage, anastomotic bleeding, surgical site infection, and intestinal obstruction) was also conducted.
Statistical Analysis
We analyzed statistically all data using the IBM SPSS Statistics for Windows, Version 22.0. (IBM Corp., Armonk, NY, USA). We used the t-test to compare the two groups’ operative time, blood loss, number of lymph nodes harvested, time to first flatus, and postoperative hospital stay, and the chi-squared (x2) test to compare general data and the incidence of postoperative complications between the two groups. A p-value of less than 0.05 was considered statistically significant.
Results
We found no significant differences between the two groups regarding patients’ general data (all p >0.05), rendering them comparable (Table 1).
Surgery was completed successfully in both groups. The operative time was recorded as 181.82 ± 14.84 minutes for the study group and 155.75 ± 17.86 minutes for the control group, with a statistically significant difference (t =5.736, p =0.00). The mean intraoperative blood loss was 89.32 ± 47.62 and 94.58 ± 42.65 ml (t =-0.436, p =0.664), the number of lymph nodes harvested was 23.05 ± 5.08 and 23.50 ± 5.57 (t =-0.311, p =0.757), the time to first flatus was 4.36 ± 1.01 and 3.93 ± 1.09 days (t =1.507, p =0.137), and the postoperative hospital stay was 16.36 ± 3.26 and 16.17±2.54 days (t =0.257, p =0.798), for the study group and control group, respectively, with no significant differences (Table 2).
In the study group, there was one postoperative intestinal obstruction and two cases of surgical site infection, while in the control group, there were two cases of surgical site infection postoperatively. There was also no significant difference in postoperative complications between the two groups, including anastomotic leakage, anastomotic bleeding, surgical site infection, and intestinal obstructio (x2 =1.132, p =0.287) (Table 3).
Discussion
Colon cancer stands as a prevalent malignancy within the digestive tract in China, holding the third position in both incidence and mortality rates among various malignancies. Furthermore, an upward trajectory in its prevalence is observed annually. Right-sided colon cancer accounts for about 30 % of all colon cancers. For right-sided colon cancer without distant metastasis, surgical treatment is the preferred treatment option. In recent years, laparoscopic techniques have rapidly developed and are characterized by minimal invasiveness and quick recovery. Several randomized controlled clinical trials have confirmed that the short-term and medium-to-long-term effects of laparoscopic colon cancer radical surgery are comparable to those of open surgery15,16. International guidelines advocate laparoscopic colon cancer radical surgery as the standard procedure for the management of colon cancer.
The surgical treatment of colon cancer with laparoscopy includes three methods: total laparoscopy, laparoscopic-assisted, and hand-assisted laparoscopy17. Among these, laparoscopic-assisted surgery is the most widely used in colon cancer surgeries. This approach entails the initial laparoscopic mobilization of the tumor, surrounding mesentery, lymph nodes, and vessels, followed by the creation of an abdominal-assisted small incision to accomplish tumor resection and anastomosis. Applying this surgical technique necessitates pre-placement of trocars in the abdomen for introducing CO2, establishing a specific pneumoperitoneum pressure (ranging from 12 to 15 mmHg) to ensure an adequate operating space within the abdominal cavity18. According to available data, 8-20 % of patients diagnosed with colon cancer present with acute intestinal obstruction19. The presence of intestinal obstruction results in the dilatation of the proximal colon and small intestine in close proximity to the tumor, leading to the accumulation of trapped air and fluid that subsequently causes a reduction in the available space within the abdominal cavity. This hinders the establishment of pneumoperitoneum and limits surgical maneuverability. Even with laparoscopic surgery, the risk of iatrogenic injury is extremely high. Often, only exploratory procedures can be performed, and it is impossible to complete the entire operation, thus requiring a transition to open surgery or direct adoption of traditional exploratory laparotomy.
To avoid limited exposure of the surgical field and collateral damage, some researchers have explored alternatives. For instance, a self-expanding metal stent is inserted into the obstruction site through the rectum using endoscopic or fluoroscopic techniques to expand the obstructed bowel. Once the obstruction symptoms are relieved, laparoscopic surgery is performed at a later time20,21, followed by deferred laparoscopic surgery. This approach achieves results comparable to open surgery while avoiding the risk of a secondary surgical procedure following an emergency colostomy. However, intestinal stent placement is more suited for the left-sided colon or rectum. Guo et al attempted to treat malignant intestinal obstruction in the ileocecal area with transnasal insertion of a 3-meter-long intestinal obstruction catheter placed into the small intestine under X-ray fluoroscopy. The catheter, aided by the gravity of the water-filled balloon at its tip, moved along the digestive tract with peristalsis, decompressing the intestine as it progresses to the distal ileum. After effective intestinal decompression, laparoscopic surgery was then performed. They pursued elective laparoscopic right hemicolectomy, deeming this approach safe and viable22. Nevertheless, the thin diameter of the transnasal intestinal obstruction catheter may lead to potential challenges, as the distal intestinal contents, often thick in nature, have a propensity to obstruct the decompression tube. In recent years, some researchers have used a hand-assisted laparoscopic approach, involving an auxiliary incision in the abdomen23. This incision enables the surgeon to manually assist during the surgical procedure manually, subsequently allowing for the insertion of laparoscopic instruments to conclude the surgery. Compared to conventional open surgery, this technique results in less trauma, quicker intestinal function recovery, and a lower wound infection rate. Consequently, it is a reliable option and serves as a bridge between traditional open surgery and conventional laparoscopic surgery. Nevertheless, hand-assisted laparoscopy necessitates specialized equipment such as the costly “lap disc”. Given that this technique involves the introduction of a hand into the abdomen, the surgical incision is larger compared to conventional laparoscopic surgery. The presence of the hand within the abdomen imposes limitations on the surgical field, impeding the seamless progression of the operation. The surgeon’s non-dominant hand remains consistently confined within the lap disc throughout the procedure, leading to fatigue. Additionally, the relatively low prevalence of this surgical technique makes it challenging to promote on a larger scale.
In this study, an initial auxiliary minor incision of five to seven cm was executed in the upper abdomen to gain access into the abdominal cavity. Subsequently, the small intestine was extricated through a surgically created port located at the terminal portion of the ileum. A suction device was inserted to facilitate decompression of the small intestine and ascending colon. In instances where the intestinal contents exhibited a thickness that hindered extraction, a practical approach involved making an incision in the ileum to facilitate decompression. This method eliminates the need for an intestinal obstruction catheter or stent, proving to be cost-effective. Following the completion of intestinal decompression, the auxiliary incision is closed using a surgical rubber glove. The surgical procedure was then carried out using the standard midline technique for laparoscopic operation. At this juncture, due to a notable reduction in the contents of the intestinal tract, there was an expansion of the intra-abdominal space, facilitating the successful execution of the surgical procedure, akin to cases lacking obstruction. This approach mitigated the potential harm to abdominal organs that may arise from laparoscopic surgery, as well as greater trauma associated with conventional open surgery. Compared to the control group, the study group exhibited a statistically significant increase in operative time that could be attributed to the intestinal incision and decompression requirement. There were no significant differences between the two groups regarding intraoperative blood loss, number of lymph nodes harvested, time to first flatus, and duration of hospital stay. Further comparison of postoperative complications between the two groups revealed that the study group did not experience a significant increase in postoperative complications.
This study has several limitations. The small sample size and single-center, retrospective design may introduce certain biases into the data. The limited sample size also restricts the generalizability of the results and increases the likelihood of sampling bias, potentially leading to inaccurate or skewed findings. Additionally, retrospective studies rely on existing data and records, which may contain missing information or documentation errors, affecting the reliability of the results. Since data were collected after the events occurred, it is not possible to standardize procedures or interventions as in prospective studies.
Conclusion
To summarize, performing a laparoscopic right hemicolectomy following abdominal-assisted small incision intestinal decompression effectively resolves the issue of insufficient abdominal capacity resulting from proximal intestinal dilation caused by obstruction. This technique yields minimal surgical trauma and is cost-effective, safe, and reliable, achieving short-term outcomes comparable to standard laparoscopic surgery. If postoperative adjuvant therapy (such as chemotherapy) is needed, it can be initiated sooner, potentially helping to slow tumor progression and improve survival rates. However, further comparative studies with relevant control groups, such as decompression via stents or nasointestinal tubes followed by surgery, are needed to evaluate this approach’s relative advantages and disadvantages.
Conflict of interest
The authors declare no conflicts of interest regarding this work.
References
- Arnold M, Abnet CC, Neale RE, Vignat J, Giovannucci EL, McGlynn KA, et al. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology. 2020; 159: 335-349.e15.
- Zhang HC, Deng SH, Pi YN, Guo JN, Xi H, Shi X, et al. Identification and Validation in a Novel Quantification System of Ferroptosis Patterns for the Prediction of Prognosis and Immunotherapy Response in Left- and Right-Sided Colon Cancer. Front Immunol. 2022; 13: 855849.
- Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019; 394: 1467-1480.
- Bourakkadi Idrissi M, El Bouhaddouti H, Mouaqit O, Ousadden A, Ait Taleb K, Benjelloun EB. Left-Sided Colon Cancer and Right-Sided Colon Cancer: Are They the Same Cancer or Two Different Entities? Cureus. 2023; 15: e37563.
- Lee MS, Menter DG, Kopetz S. Right Versus Left Colon Cancer Biology: Integrating the Consensus Molecular Subtypes. J Natl Compr Canc Netw. 2017; 15: 411-419.
- Yoo RN, Cho HM, Kye BH. Management of obstructive colon cancer: Current status, obstacles, and future directions. World J Gastrointest Oncol. 2021; 13: 1850-1862.
- Vilsan J, Maddineni SA, Ahsan N, Mathew M, Chilakuri N, Yadav N, et al. Open, Laparoscopic, and Robotic Approaches to Treat Colorectal Cancer: A Comprehensive Review of Literature. Cureus. 2023; 15: e38956.
- Cirocchi R, Cesare Campanile F, Di Saverio S, Popivanov G, Carlini L, Pironi D, et al. Laparoscopic versus open colectomy for obstructing right colon cancer: A systematic review and meta-analysis. J Visc Surg. 2017; 154: 387-399.
- Mare H, Tjhin W. Successful Laparoscopic Management of Pericaecal Hernia Causing Small Bowel Obstruction. Cureus. 2023; 15: e34663
- Boeding JRE, Elferink MAG, Tanis PJ, de Wilt JHW, Gobardhan PD, Verhoef C, et al. Surgical treatment and overall survival in patients with right-sided obstructing colon cancer-a nationwide retrospective cohort study. Int J Colorectal Dis. 2023; 38: 248.
- Boeding JRE, Ramphal W, Rijken AM, Crolla RMPH, Verhoef C, Gobardhan PD, et al. Systematic Review Comparing Emergency Resection and Staged Treatment for Curable Obstructing Right-Sided Colon Cancer. Ann Surg Oncol. 2021; 28: 3545-3555.
- Bellio H, Fumet JD, Ghiringhelli F. Targeting BRAF and RAS in Colorectal Cancer. Cancers (Basel). 2021; 13: 2201.
- Warschkow R, Sulz MC, Marti L, Tarantino I, Schmied BM, Cerny T, et al. Better survival in right-sided versus left-sided stage I – III colon cancer patients. BMC Cancer. 2016; 16: 554.
- Monahan BV, Patel T, Poggio JL. Stage IV Colorectal Cancer at Initial Presentation versus Progression during and after Treatment, Differences in Management: Management Differences for Initial Presentation versus Progression of Disease after Initial Treatment. Clin Colon Rectal Surg. 2023; 37: 108-113.
- Colon Cancer Laparoscopic or Open Resection Study Group; Buunen M, Veldkamp R, Hop WC, Kuhry E, Jeekel J, et al. Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol. 2009; 10: 44-52.
- Kitano S, Inomata M, Mizusawa J, Katayama H, Watanabe M, Yamamoto S, et al. Survival outcomes following laparoscopic versus open D3 dissection for stage II or III colon cancer (JCOG0404): a phase 3, randomised controlled trial. Lancet Gastroenterol Hepatol. 2017; 2: 261-268.
- Mocan L. Laparoscopic surgery for the treatment of colon cancer: the new standard? Eur Rev Med Pharmacol Sci. 2021; 25: 4228-4235.
- Sato K, Imaizumi K, Kasajima H, Kurushima M, Umehara M, Tsuruga Y, et al. Short-term outcomes of extracorporeal colo-colonic triangular anastomosis versus functional end-to-end anastomosis in laparoscopic-assisted surgery for left-sided colon cancer: a propensity score matching analysis. Langenbecks Arch Surg. 2022; 407: 747-757.
- Yang KM, Jeong MJ, Yoon KH, Jung YT, Kwak JY. Oncologic outcome of colon cancer with perforation and obstruction. BMC Gastroenterol. 2022; 22: 247.
- Kaplan J, Strongin A, Adler DG, Siddiqui AA. Enteral stents for the management of malignant colorectal obstruction. World J Gastroenterol. 2014; 20: 13239-13245.
- CReST Collaborative Group. Colorectal Endoscopic Stenting Trial (CReST) for obstructing left-sided colorectal cancer: randomized clinical trial. Br J Surg. 2022; 109: 1073-1080.
- Guo YT, Du HT, Li DC. Placement of transnasal ileus tube combined with laparoscopy in the treatment of ileocecal malignant intestinal obstruction. J Med Imaging. 2021; 31: 1922-1924.
- Li Z, Li D, Jie Z, Zhang G, Liu Y. Comparative Study on Therapeutic Efficacy Between Hand-Assisted Laparoscopic Surgery and Conventional Laparotomy for Acute Obstructive Right-Sided Colon Cancer. J Laparoendosc Adv Surg Tech A. 2015; 25: 548-554.