RESEARCH ARTICLE
Hippokratia 2019, 23(1): 9-14
Kleisarchaki AN, Papadopoulou-Legbelou K, Kotanidou EP, Kotanidis CP, Eboriadou-Petikopoulou M, Galli-Tsinopoulou A.
4th Department of Paediatrics, Medical School, Faculty of Health Sciences, Aristotle University of Thessaloniki, Papageorgiou General Hospital, Thessaloniki, Greece
![]()
Abstract
Background: Experimental and clinical studies have shown the cardio-protective, anti-inflammatory, and anti-atherosclerotic actions of vitamin D.
Material and Methods: We aimed to investigate a possible correlation between vitamin D status and heart geometry using echocardiographic parameters of the left ventricle in youngsters with type 1 diabetes mellitus (T1D). Seventy-eight pediatric patients (aged 13.47 ± 2.86 years) with T1D of more than two years duration and 74 healthy controls (aged 12.04 ± 2.79 years) were enrolled in this case-control study. Anthropometric parameters were recorded, vitamin D and parathormone serum levels were measured, and trans-thoracic echocardiographic study was performed.
Results: Vitamin D deficiency was found in 74 % T1D patients and in 72 % of the controls, while parathormone levels were normal in both groups. T1D patients presented significantly higher values of interventricular septal thickness at diastole (IVSD) compared to controls (0.76 ± 0.16 cm vs 0.71 ± 0.14 cm, p =0.043). All other echocardiographic parameters did not exhibit significant differences between patients and controls. The diastolic function of the left ventricle (LV) was normal in both groups. After sub-grouping, the participants according to the deficiency or not of vitamin D, only patients with T1D and low vitamin D levels had increased values of IVSD compared to controls (0.78 ± 0.17 vs 0.71 ± 0.14, p =0.008). Patients with T1D and normal vitamin D levels presented similar values of IVSD compared to controls (0.71 ± 0.12 vs 0.73 ± 0.15, p =NS).
Conclusions: Children and adolescents with T1D and normal vitamin D levels do not exhibit changes in LV dimensions or diastolic function, except for increased IVSD, compared to controls. Larger and longitudinal studies are required to confirm and consolidate this finding. HIPPOKRATIA 2019, 23(1): 9-14.
Keywords: Vitamin D deficiency, diabetes type 1, echocardiography, child, adolescent
Corresponding author: Kyriaki Papadopoulou-Legbelou, MD, PhD, Associate Professor in Paediatrics-Paediatric Cardiology, 4th Department of Pediatrics, Medical School, Aristotle University of Thessaloniki “Papageorgiou” General Hospital, Ring Road Nea Efkarpia, Thessaloniki 56403, Greece, tel: +302310991463, fax: +302313323918, e-mail: kelipap@gmail.com; kpapadopoulou@auth.gr
Introduction
Vitamin D plays a crucial role in maintaining bone health and regulating calcium homeostasis1. The identification of the vitamin D receptor (VDR) in a number of different cells and tissues (cardiomyocytes, pancreatic beta-cells, nerve cells, endothelial cells, immune cells, osteoblasts), suggests that vitamin D exerts a wide range of actions in extra-skeletal tissues2. Data from various experimental and clinical studies have shown the cardio-protective3,4, anti-inflammatory5, and anti-atherosclerotic actions of vitamin D6-8.
Vitamin D deficiency (VDD) has been reported to be associated with a variety of cardiovascular and metabolic disorders, such as hypertension, insulin resistance, metabolic syndrome, diabetes mellitus, peripheral vascular disease, and congestive heart failure9-15. Studies in adults have shown that patients with type 1 diabetes (T1D) and VDD exhibit left ventricular hypertrophy and diastolic dysfunction16,17. Furthermore, substitution therapy with vitamin D has been reported to result in blood pressure reduction in humans and can also reverse cardiac hypertrophy in rats18,19.
These data support the existence of a possible mechanistic connection between VDD and cardiovascular disease. However, most studies focus on adults, and data on children and adolescents with VDD is limited. The aim of the present study was to investigate the possible correlation between serum vitamin D levels and echocardiographic parameters of the left ventricle (LV) in children and adolescents with T1D.
Materials and Methods
Seventy-eight consecutive pediatric patients (43 boys), with T1D (mean age of 13.47 ± 2.86 years), were enrolled in the case-control study during the same autumn-winter seasonal period. These young patients, attended the pediatric Diabetes outpatient unit, of the 4th department of Pediatrics of the Aristotle University of Thessaloniki, at “Papageorgiou” General Hospital, from October 2012 to March 2015. The inclusion criteria were: pediatric patients who suffered from T1D for more than two years, Caucasian race, age range between 7 and 18 years old, and negative family history for cardiac malformation or cardiac disease. The exclusion criteria for the study were the presence of obesity, acute illness, diabetic complications, as well as the administration of any medication other than insulin.
The control group consisted of 80 children/adolescents with normal weight [body mass index (BMI) <85th percentile for age and gender], who had volunteered or came from those who attended the general Pediatrics outpatient clinic. Three of them were excluded from the study due to hyperglycemia and three due to infection. Finally, seventy-four healthy children/adolescents (38 boys), with mean age of 12.04 ± 2.79 years, were enrolled. Acute or chronic disease, obesity, and T1D or other autoimmune diseases were the exclusion criteria for the control group.
A required sample size of 126 participants (63 for each group) was calculated (http://statulator.com/SampleSize/ss2M.html; sample size calculator for comparing two independent means) in order to achieve a power of 80 % and a level of significance of 5 % (two sided), for detecting a true difference of -0.1099 units in means between the study group and the control.
All participants underwent a systematic clinical evaluation, including anthropometric measurements, by the same pediatrician. BMI was calculated using the formula: body weight (kilograms)/height (meters)2. Blood pressure was measured with the participant in the sitting position, using the appropriate cuff size.
Glycated hemoglobin (HbA1c) was measured in a capillary blood sample in all T1D patients utilizing a specific method (DCA 2000R+ Hemoglobin A1c, Siemens, Germany). In all participants, serum levels of 25-hydroxycholecalciferol [25(OH)D] were measured by radioimmunoassay, with an automatic gamma counter (Wallac 1470 Wizard, Turku, Finland). Furthermore, parathormone levels (PTH) were measured by direct chemiluminescence (ADVIA, Centaur XTP, Siemens, USA). Levels of 25(OH)D greater than 30 ng/ml were considered normal, whereas levels below 30 ng/ml defined as VDD20.
Trans-thoracic echocardiographic study was performed in the left decubitus position using a General Electric-Vivid 3 Pro (Israel) ultrasound machine with a 5 MHz transducer. Guided by two-dimensional echocardiography short-axis view, standard M-mode parameters of LV were obtained following the recommendations of the American Society of echocardiography21. The measurements included the following parameters: left ventricular internal diameter at end-diastole and end-systole (LVIDD, LVIDS, respectively), interventricular septal thickness at diastole (IVSD), left ventricular posterior wall thickness at end-diastole (LVPWD), LV ejection fraction and fractional shortening (EF, FS), and LV mass. LV mass index (LVMI) was obtained by the following formula: LV mass/body surface area (g/m2). We also indexed LV mass by height3 in order to determine the presence of LV hypertrophy (using the 95th percentile as a cut-off)22. Measurement of left atrial diameter (LAD) was performed from M-mode parasternal short-axis view at the level of the aortic valve21. From the parasternal 4-chamber view, using Doppler echocardiography, we also estimated the LV diastolic function by measuring E wave, A wave of the mitral valve, and the E/A ratio.
The study was approved by the Ethics Committee of the School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki (decision No 2, 23/3/2016) and informed written consent was obtained from all participants’ parents or guardians.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation for normally distributed and as median (minimum-maximum in brackets) for non-normally distributed. Kolmogorov-Smirnov and Shapiro-Wilk tests were used to examine the normality of distributions based on the size of the groups under comparison. Comparison of variables between two groups was performed with either Student’s t-test for normally distributed, or Mann-Whitney U-test for non-normally distributed variables. Categorical variables among groups were compared using the chi-squared test. A comparison of means among three or more groups was conducted by one-way analysis of variance. For multiple comparisons, Bonferroni posthoc tests were applied, after correction for the level of significance. Correlation between variables was assessed by Spearman’s rank correlation coefficient. Data were analyzed using IBM SPSS Statistics for Windows, Version 19 (IBM Corp., Armonk, NY). All tests were two-sided, and α was set at 0.05.
Results
Demographic and basic clinical characteristics of the participants are summarized in Table 1. In both groups, PTH levels ranged within the normal range. However, low vitamin D levels were found in both T1D patients (58/78, 74 %) as well as in the control group (53/74, 72 %) (Table 1). The mean value of HbA1c was 8.09 ± 1.13 %, and the mean duration of T1D was 6.83 ± 3.29 years.
Individuals with T1D presented significantly higher levels of IVSD compared to controls (0.76 ± 0.16 cm vs 0.71 ± 0.14 cm, p =0.043) (Table 2, Figure 1). All other mean values of echocardiographic parameters of the left ventricle did not exhibit significant differences between the two groups (Table 2). The diastolic function of the left ventricle was also normal in the two groups with no statistically significant difference (Table 2).
When participants were sub-grouped according to the presence or not of VDD, mean values of anthropometric and demographic characteristics did not differ between patients and controls. Comparing all the echocardiographic parameters, mean values did not differ significantly between children with or without VDD, except for IVSD (Figure 1). Patients with T1D had increased mean values of IVSD compared to controls only in the subgroup of low vitamin D levels (0.78 ± 0.17 and 0.71 ± 0.14, respectively, p =0.008). On the other hand, patients with T1D and normal vitamin D levels presented similar values of IVSD compared to controls (0.71 ± 0.12 and 0.73 ± 0.15, respectively, p =0.632).

Figure 1: Boxplot of the interventricular septal thickness end diastole (IVSD) values in type 1 diabetes (T1D) children/adolescents and controls; A) Comparison between T1D and controls in total sample; B) Comparison between T1D and controls in the vitamin D deficiency subgroup; C) Comparison between T1D and controls in the subgroup without vitamin D deficiency. TIDM: Type 1 diabetes mellitus, IVSD: Interventricular septal thickness end diastole.
After the application of correlation analysis, it was revealed that vitamin D levels presented a significant positive correlation with LVMI (r =0.164, p =0.043) and LV mass/height3 (r =0.162, p =0.046) (Figure 2). Additionally, vitamin D levels presented a statistical trend correlation with diabetes duration, in a negative manner (r =-0.206, p =0.071).

Figure 2: Correlation between vitamin D levels and A) left ventricle (LV) mass index and B) LV mass/height3. LV: Left Ventricle.
Furthermore, diabetes duration showed significantly positive correlations to a wide variety of cardiac indexes: IVSD (r =0.372, p =0.001), LV mass (r =0.332, p =0.003), LVMI (r =0.231, p =0.042), and LAD (r =0.383, p =0.001) (Figure 3). Finally, HbA1c levels exhibited a significant positive correlation to diabetes duration (r =0.26, p =0.021), a statistical trend to correlate positively to LAD values (r =0.222, p =0.055), and a negative correlation to vitamin D levels without reaching a statistically significant level (r =-0.163, p =0.15).
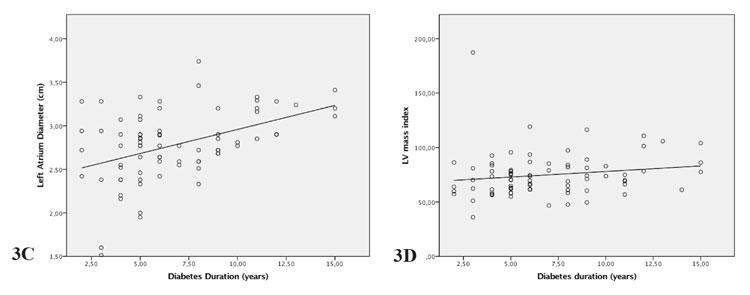
Figure 3: Correlation between diabetes duration and A) interventricular septal thickness end diastole (IVSD), B) left ventricle (LV) mass, C) left atrial diameter, D) LV mass index in type 1 diabetes children/adolescents. IVSD: Interventricular septal thickness end diastole, LV: Left ventricle.
Discussion
The present study shows that children and adolescents with T1D and VDD do not have changes in LV wall dimensions or diastolic function compared to controls, except for IVSD. Septal hypertrophy has been described as an early echocardiographic finding of left ventricular hypertrophy in childhood obesity23,24.
Although a correlation between VDD and diabetes in adults has been reported in multiple studies, there are only a few studies investigating the incidence of VDD in children and adolescents with T1D and its impact on cardiometabolic complications17,25-27.
In the present study, the prevalence of low vitamin D levels was similarly high between the groups of the overall cohort. This finding is in agreement with the study by Wood et al28. However, after the division of the participants into subgroups, it was revealed that low vitamin D levels were associated with a statistically increased mean value of IVSD only in children and adolescents with T1D compared with controls. This is a very interesting finding, but it should be confirmed by further larger studies.
Pandit et al also found that interventricular septal thickness was significantly increased in a group of VDD adult population compared to a group with normal vitamin D levels29. Another study in adults showed that patients with VDD had higher LVIDS, IVSD, LVPWD, and LV mass compared to patients with normal vitamin D levels30. The authors claim that VDD diminish the protective effect of vitamin D from fibrosis, myocardial thickening, and anti-apoptosis17.
Diastolic function of the LV was normal in our patients. This finding is consistent with previous studies in adults on the same topic27,29. Nevertheless, diastolic dysfunction has been described in young patients with T1D, using conventional and novel methods, such as tissue Doppler imaging31-35.
Contrary to diastolic function, LV systolic function was not reported to be impaired in most studies35. However, Di Cori et al using highly sensitive echocardiographic techniques demonstrated the presence of systolic dysfunction in young adults with well-controlled T1D36.
The duration of T1D and HbA1c levels have been correlated with diastolic dysfunction in T1D patients31,37. Diastolic dysfunction may be an early alteration, that precedes systolic dysfunction34,38. The presence of left ventricular systolic and/or diastolic dysfunction in T1D patients has been described as “diabetic cardiomyopathy”, which is related to metabolic control and the duration of the disease38,39.
In the present study, there was neither systolic nor diastolic dysfunction. The above finding can be attributed to the participants’ sufficient glycemic control (since the 75th percentile of the HbA1c variable was 8.7 %), or to the short duration of the disease (in 75 % of the study population, disease duration was less than nine years). As a result, we did not find echocardiographic features of diabetic cardiomyopathy in our T1D patients.
Furthermore, in this study, vitamin D levels had a significant positive correlation with LVMI and LV mass/height3. Other studies also showed a similar correlation between vitamin D levels and LV mass and LV wall thickness27,40. With regard to HbA1c, we found a negative correlation with vitamin D levels, without reaching a statistically significant level. One more study failed to observe a significant correlation, but other more recent studies found a statistically significant negative correlation between vitamin D levels and HbA1c levels26,41,42.
Summarizing the results of the present study, we conclude that an incipient left ventricular hypertrophy could be a unique and early sign of cardiac structural changes, which could potentially lead to cardiomyopathy in children and adolescents with T1D and low vitamin D levels. Therefore, routine measurement of circulating vitamin D levels is recommended in T1D youngsters, not only to achieve good bone mass but also to avoid a potential early onset of cardiac dysfunction.
Conflict of interest
Authors declare no conflict of interest.
Acknowledgments
Authors would like to thank the patients (and their parents/guardians) for their participation in the study.
References
1. Holick MF. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Dis.2017; 18: 153-165.
2. Gil Á, Plaza-Diaz J, Mesa MD. Vitamin D: Classic and Novel Actions. Ann Nutr Metab. 2018; 72: 87-95.
3. Liss Y, Frishman W. Vitamin D: a cardioprotective agent? Cardiol Rev. 2012; 20: 38-44.
4. Schnatz PF, Manson JE. Vitamin D and cardiovascular disease: an appraisal of the evidence. Clin Chem. 2014; 60: 600-609.
5. Vojinovic J. Vitamin D receptor agonists’ anti-inflammatory properties. Ann N Y Acad Sci. 2014; 1317: 47-56.
6. Kienreich K, Grubler M, Tomaschitz A, Schmid J, Verheyen N, Rutters F, et al. Vitamin D, arterial hypertension & cerebrovascular disease. Indian J Med Res. 2013; 137: 669-679.
7. Pilz S, Tomaschitz A, Ritz E, Pieber TR. Vitamin D status and arterial hypertension: a systematic review. Nat Rev Cardiol. 2009; 6: 621-630.
8. Brewer LC, Michos ED, Reis JP. Vitamin D in atherosclerosis, vascular disease, and endothelial function. Curr Drug Targets. 2011; 12: 54-60.
9. Forman JP, Giovannucci E, Holmes MD, Bischoff-Ferrari HA, Tworoger SS, Willett WC, et al. Plasma 25-hydroxyvitamin D levels and risk of incident hypertension. Hypertension. 2007; 49: 1063-1069.
10. Berridge MJ. Vitamin D deficiency and diabetes. Biochem J. 2017; 474: 1321-1332.
11. Chen LW, Chien CH, Kuo SF, Yu CY, Lin CL, Chien RN. Low vitamin D level was associated with metabolic syndrome and high leptin level in subjects with nonalcoholic fatty liver disease: a community-based study. BMC Gastroenterol. 2019; 19: 126.
12. Yuan J, Jia P, Hua L, Xin Z, Yang JK. Vitamin D deficiency is associated with risk of developing peripheral arterial disease in type 2 diabetic patients. BMC Cardiovasc Disord. 2019; 19: 145.
13. Pilz S, März W, Wellnitz B, Seelhorst U, Fahrleitner-Pammer A, Dimai HP, et al. Association of vitamin D deficiency with heart failure and sudden cardiac death in a large cross-sectional study of patients referred for coronary angiography. J Clin Endocrinol Metab.2008; 93: 3927-3935.
14. Saponaro F, Marcocci C, Zucchi R. Vitamin D status and cardiovascular outcome. J Endocrinol Invest. 2019; 42: 1285-1290.
15. Bouillon R. Vitamin D and cardiovascular disorders. Osteoporos Int. 2019; 30: 2167-2181.
16. Yoldaş T, Örün UA, Sagsak E, Aycan Z, Kaya Ö, Özgür S, et al. Subclinical left ventricular systolic and diastolic dysfunction in type 1 diabetic children and adolescents with good metabolic control. Echocardiography. 2018; 35: 227-233.
17. Iso T, Takahashi K, Yazaki K, Ifuku M, Nii M, Fukae T, et al. In-Depth Insight Into the Mechanisms of Cardiac Dysfunction in Patients With Type 1 Diabetes Mellitus Using Layer-Specific Strain Analysis. Circ J. 2019; 83: 1330-1337.
18. Rai V, Agrawal DK. Role of Vitamin D in Cardiovascular Diseases. Endocrinol Metab Clin North Am. 2017; 46: 1039-1059.
19. Bodyak N, Ayus JC, Achinger S, Shivalingappa V, Ke Q, Chen YS, et al. Activated vitamin D attenuates left ventricular abnormalities induced by dietary sodium in Dahl salt-sensitive animals. Proc Natl Acad Sci U S A. 2007; 104: 16810-16815.
20. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011; 96: 1911-1930.
21. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18: 1440-1463.
22. Daniels SR, Kimball TR, Morrison JA, Khoury P, Meyer RA. Indexing left ventricular mass to account for differences in body size in children and adolescents without cardiovascular disease. Am J Cardiol.1995; 76: 699-701.
23. Sivanandam S, Sinaiko AR, Jacobs DR Jr, Steffen L, Moran A, Steinberger J. Relation of increase in adiposity to increase in left ventricular mass from childhood to young adulthood. Am J Cardiol. 2006; 98: 411-415.
24. Brady TM. The Role of Obesity in the Development of Left Ventricular Hypertrophy Among Children and Adolescents. Curr Hypertens Rep. 2016; 18: 3.
25. Littorin B, Blom P, Schölin A, Arnqvist HJ, Blohmé G, Bolinder J, et al. Lower levels of plasma 25-hydroxyvitamin D among young adults at diagnosis of autoimmune type 1 diabetes compared with control subjects: results from the nationwide Diabetes Incidence Study in Sweden (DISS). Diabetologia. 2006; 49: 2847-2852.
26. Chakhtoura M, Azar ST. The role of vitamin d deficiency in the incidence, progression, and complications of type 1 diabetes mellitus. Int J Endocrinol. 2013; 2013: 148673.
27. Al Shaikh A, Al Zahrani AM. Impact of Vitamin D Status on Cardiometabolic Complications among Children and Adolescents with Type 1 Diabetes Mellitus. J Clin Res Pediatr Endocrinol. 2016; 8: 48-54.
28. Wood JR, Connor CG, Cheng P, Ruedy KJ, Tamborlane WV, Klingensmith G, et al. Vitamin D status in youth with type 1 and type 2 diabetes enrolled in the Pediatric Diabetes Consortium (PDC) is not worse than in youth without diabetes. Pediatr Diabetes. 2016; 17: 584-591.
29. Pandit A, Mookadam F, Boddu S, Aryal Pandit A, Tandar A, Chaliki H, et al. Vitamin D levels and left ventricular diastolic function. Open Heart. 2014; 1: e000011.
30. Abdel Rahman MA, Galal H, Omar AMS. Correlation between serum vitamin D level and cardiac function: Echocardiographic assessment. Egypt Heart J. 2015; 67: 299-305.
31. Pilz S, Henry RM, Snijder MB, van Dam RM, Nijpels G, Stehouwer CD. Vitamin D deficiency and myocardial structure and function in older men and women: The Hoorn Study. J Endocrinol Invest. 2010; 33: 612-617.
32. Ozdemir O, Koksoy AY, Bulus AD, Andiran N, Yagli E. The effects of type 1 diabetes mellitus on cardiac functions in children: evaluation by conventional and tissue Doppler echocardiography. J Pediatr Endocrinol Metab. 2016; 29: 1389-1395.
33. Khattab AA, Soliman MA. Biventricular function and glycemic load in type 1 diabetic children: Doppler tissue-imaging study. Pediatr Cardiol. 2015; 36: 423-431.
34. Brunvand L, Fugelseth D, Stensaeth KH, Dahl-Jørgensen K, Margeirsdottir HD. Early reduced myocardial diastolic function in children and adolescents with type 1 diabetes mellitus a population-based study. BMC Cardiovasc Disord. 2016; 16: 103.
35. Schannwell CM, Schneppenheim M, Perings S, Plehn G, Strauer BE. Left ventricular diastolic dysfunction as an early manifestation of diabetic cardiomyopathy. Cardiology. 2002; 98: 33-39.
36. Di Cori A, Di Bello V, Miccoli R, Talini E, Palagi C, Delle Donne MG, et al. Left ventricular function in normotensive young adults with well-controlled type 1 diabetes mellitus. Am J Cardiol. 2007; 99: 84-90.
37. Hensel KO, Grimmer F, Roskopf M, Jenke AC, Wirth S, Heusch A. Subclinical Alterations of Cardiac Mechanics Present Early in the Course of Pediatric Type 1 Diabetes Mellitus: A Prospective Blinded Speckle Tracking Stress Echocardiography Study. J Diabetes Res. 2016; 2016: 2583747.
38. Jia G, Whaley-Connell A, Sowers JR. Diabetic cardiomyopathy: a hyperglycaemia- and insulin-resistance-induced heart disease. Diabetologia. 2018; 61: 21-28.
39. Adal E, Koyuncu G, Aydın A, Çelebi A, Kavunoǧlu G, Çam H. Asymptomatic cardiomyopathy in children and adolescents with type 1 diabetes mellitus: association of echocardiographic indicators with duration of diabetes mellitus and metabolic parameters. J Pediatr Endocrinol Metab. 2006; 19: 713-726.
40. Ameri P, Canepa M, Milaneschi Y, Spallarossa P, Leoncini G, Giallauria F, et al. Relationship between vitamin D status and left ventricular geometry in a healthy population: results from the Baltimore Longitudinal Study of Aging. J Intern Med. 2013; 273: 253-262.
41. Wierzbicka E, Szalecki M, Pludowski P, Jaworski M, Brzozowska A. Vitamin D status, body composition and glycemic control in Polish adolescents with type 1 diabetes. Minerva Endocrinol. 2016; 41: 445-455.
42. Savastio S, Cadario F, Genoni G, Bellomo G, Bagnati M, Secco G, et al. Vitamin D Deficiency and Glycemic Status in Children and Adolescents with Type 1 Diabetes Mellitus. PLoS One. 2016; 11: e0162554.