ORIGINAL ARTICLE
Hippokratia 2014, 18(2):116-119
Tsikopoulos G, Asimakidou M, Smaropoulos E, Farmakis K, Klokkaris A
Paediatric Surgery Department, Hippokration General Hospital of Thessaloniki, Thessaloniki, Greece
![]()
Abstract
Aim: To assess the difference in aesthetic result after a non-religious circumcision with classic Johnston’s technique and a new proposed technique.
Materials and methods: A total of 76 children were circumcised (not for religious purposes) in a period of 6 years using the classic Johnston’s technique (50 patients) and a new proposed technique (26 patients). Parents of circumcised children were interviewed three months after the operation. The aesthetic result was scored by both the parents and the patients as bad, acceptable, good or very good. Scores between the two groups were compared.
Results: No major complications were encountered. The aesthetic result score between the two groups had a statistically significant difference (Mann Whitney U Test, p<0.0005). Children being circumcised with the new technique and their parents were more satisfied with the aesthetic result three months after the operation.
Conclusions: In communities in which religious circumcisions are being performed relatively rare, the aesthetic result of a classic method may seem awkward to the patient and his family. Therefore, circumcision being performed for non religious reasons necessitates an acceptable aesthetic result. Our technique fulfills this prerequisite.
Key words: circumcision, technique, cosmetic
Corresponding author: Tsikopoulos George, Head of Paediatric Surgery Department, Hippokration General Hospital of Thessaloniki, Konstantinoupoleos 49, 546 42, Thessaloniki, Greece, tel: +302310892338, fax: +302310892338, e-mail: tsikop@yahoo.gr
Introduction
Circumcision is one of the commonest operations performed in children. It is usually performed for religious, social, cultural or medical reasons. In muslim and jewish societies, being circumcised is considered as a prerequisite in order “to become a man” and the expected aesthetic result is usually acceptable1. Also in countries where circumcision is performed in most men the aesthetic result is considered preferable from women2. In Greek community, where the majority of population is Christians of the Orthodox Church, circumcision is performed most commonly for medical reasons. In a society that is not familiar with the appearance of a classic circumcision, the aesthetic result of this procedure is of great importance. In such cases that the circumcision is performed for non religious reasons, the expected result is this of an uncircumcised glans.
In this article we propose a Johnston’s modification technique and we present the comparative evaluation of the conceived aesthetic result to the aesthetic result of the traditionally used Johnston’s technique.
Materials and Methods
During a six year period (2007-2012) a total of 158 operations for phimosis were performed in our pediatric surgery department. Every independent case presented with a typical appearance of a non-retractable foreskin. In most of them the cause was a scar due to a previous forcible retraction(s) of the skin from parents and/or physicians. The appearance of the foreskin and glans was normal whilst in two cases balanitis xerotica obliterans was noticed (Figure 1).

Figure 1: Typical appearance of a phimosis’ case, with non-retractable foreskin.
For the 82 of them a dorsal slit was adequate, whilst for the rest 76 a circumcision was performed. From the 76 circumcised patients 50 were treated with the traditional Johnston’s technique and 26 were operated with a newly proposed method.
The technique consists of the following steps: a. freeing the foreskin from the glans after dorsal slit, b. frenulotomy, c. encircling incision 5mm from the coronal sulcus and excision of the distal inner aspect of the foreskin, d. minor excision of the prepucial skin which includes the fibrous tissue in order to achieve a redundant outer layer of the skin and e. re-aproximation of the traumatic edges with absorbable interrupted sutures 5/0 (Figures 2, 3, 4).
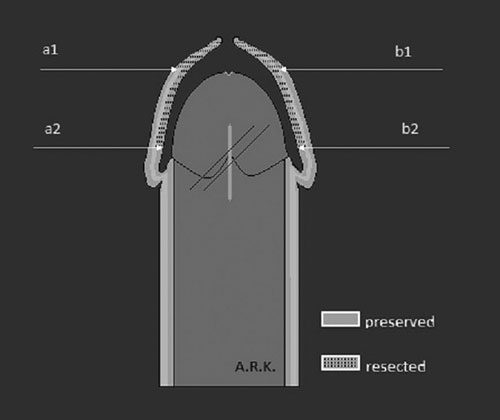
Figure 2: Schematic representation of the glans. The part of the preputial skin that is resected is marked as a dotted area. The outer layer is preserved and, after approximation of the free edges (a1 with a2 and b1 with b2), it moves inwards giving to the glans an almost normal appearance.
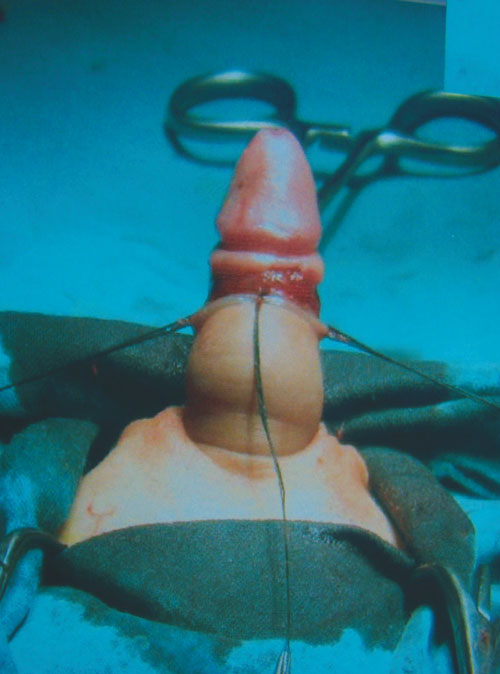
Figure 3: Operative picture of the previous schematic analysis.

Figure 4: Picture demonstrating the final operative result.
Three months postoperatively a routine examination was performed in every patient. All patients attended the reexamination appointment (attendance rate 100%). Kids over 10 years of age (47 out of 76) were asked about individual aesthetic result in combination with parental aspect whilst for the rest, only parental opinion was scored. The satisfaction grade was recorded as a single score from both parents and patients (when possible) after a standard interview from the same interviewer. When voting was conflicting (patient VS parents), votes were scored as different ones. The aesthetic result was scored as bad, acceptable, good or very good. The difference in scores between the two groups was evaluated (Figures 5, 6).

Figure 5: Picture 75 days after the operation (with retracted foreskin).

Figure 6: Picture 75 days after the operation, not showing any sign of circatrisation.
Results
A total of 76 circumcised patients were encountered in the study. Their age varied from 4 to 13 years of age. The traditional Johnston’s technique was used in 50 of them and the newly proposed method was performed in 26 patients. No major postoperative complications were encountered for both methods. All patients (100%) were reexamined three months after the operation and the aesthetic result score was recorded. As the aesthetic result scores did not have a normal distribution, Mann-Whitney U Test was used to assess the differences between the two groups. Mann- Whitney U Test revealed a statistical significance in the conceived by the parents and patients aesthetic result between classic Johnston technique and the proposed technique (U=76.0, z=-6.686, p<0.0005, r=0.767). Higher satisfaction levels were observed for the newly proposed technique. Remarkably, no patient being operated with the new technique scored the aesthetic result as bad or just acceptable (Table 1).
Discussion
Worldwide there is strong ongoing debate on whether the children should be circumcised in a regular basis or not3-5. A lot of studies access the possible beneficial effect of this procedure6. It is believed that circumcision has a protective effect against urinary track infections and penile cancer7-8. Studies assessing the possible protective effect of circumcision against sexually transmitted diseases such as HPV and HIV have shown conflicting results9-11. Additionally, there is evidence that foreskin has erogenous sensitivity which is impaired with circumcision12. Finally, we should not forget that being circumcised is a procedure that produces fear and is worrisome to the child patient1.
Parents are not always informed about the procedure or its possible complications. A study conducted in Korea had shown that the information about pros and cons of circumcision may have caused a steep decline in the total number of circumcisions13. Additionally, the socioeconomic status and the educational level of parents have an implication on overall knowledge about circumcision and its benefits.
Cultural aspects influence both the decision to have a circumcision and the expectations from this procedure. When circumcision is performed for religious reasons, the cosmetic result is highly acceptable from both the parents and the patients and a bad scar is then considered a complication of the procedure1.
In countries that circumcision is not mandatory for religious reasons parents should be briefly informed about the possible complications of this procedure and the expected aesthetic result. In our department, 129 out of 158 cases were operated for non-religious beliefs. It is clear that all the rest 29 cases where submitted to a typical circumcision, following classic Johnston’s technique. Every kid over 10 years of age (47 out of 76) was asked preoperatively about any special desire for penis’s appearance and 25 out of 47 expressed a wish for an aesthetic result as close as can be to the non-circumcised penis. Our study has proven that the aesthetic result of a classic circumcision is not easily acceptable in a community like ours where religious circumcision is relatively rare.
Taking into account this controversy, circumcision should be considered always in comparison with the religious and social background of the country in general and the family in particular. Surgeons should pay attention to the possible psychological effects that the procedure and the aesthetic result may have to the patient. This is of great importance, especially when the expected result is this of an uncircumcised glans. Our newly proposed technique is shown to be highly acceptable in a community that is not familiar with the cosmetic result of a circumcision. In addition, no major side effects were encountered, making this procedure as safe as the classic Johnston’s technique. A future study should check for possible effectiveness of the new method against urinary track infections, sexually transmitted diseases and penile cancer.
Conflict of interest
Authors declare no conflict of interest regarding the present study.
References
1. Corduk N, Unlu G, Sarioglu-Buke A, Buber A, Savran B, Zencir M. Knowledge, attitude and behaviour of boys and parents about circumcision. Acta Paediatr. 2013; 102: e169-e173.
2. Weiss GN, Weiss EB. A perspective on controversies over neonatal circumcision. Clin Pediatr (Phila). 1994; 33: 726-730.
3. Gomella LG. Circumcision: a spiritual, medical or criminal act? Can J Urol. 2012; 19: 6530.
4. Updegrove KK. An evidence-based approach to male circumcision: what do we know? J Midwifery Womens Health. 2001; 46: 415-422.
5. Robinson JD, Ortega G, Carrol JA, Townsend A, Carnegie DA, Rice D, et al. Circumcision in the United States: where are we?J Natl Med Assoc. 2012; 104: 455-458.
6. Tobian AA, Gray RH, Quinn TC. Male circumcision for the prevention of acquisition and transmission of sexually transmitted infections: the case for neonatal circumcision. Arch Pediatr Adolesc Med. 2010; 164: 78-84.
7. Morris BJ, Wiswell TE. Circumcision and life time risk of urinary tract infection: a systematic review and meta-analysis. J Urol. 2013; 189: 2118-2124.
8. Sonpavde G, Pagliaro LC, Buonerba C, Dorff TB, Lee RJ, Di Lorenzo G. Penile cancer: current therapy and future directions. AnnOncol. 2013; 24: 1179-1189.
9. Albero G, Villa LL, Lazcano-Ponce E, Fulp W, Papenfuss MR, Nyitray AG, et al. Male circumcision and prevalence of genital human papilloma virus infection in men: a multinational study. BMC Infect Dis. 2013; 13: 18.
10. Siegfried N, Muller M, Volmink J, Deeks J, Egger M, Low N, et al. Male circumcision for prevention of heterosexual acquisition of HIV in men. Cochrane Database Syst Rev. 2003: CD003362.
11. Millett GA, Flores SA, Marks G, Reed JB, Herbst JH. Circumcision status and risk of HIV and sexually transmitted infections among men who have sex with men: a meta-analysis. JAMA. 2008; 300: 1674-1684.
12. Bronselaer GA, Schober JM, Meyer-Bahlburg HF, T’Sjoen G, Vlietinck R, Hoebeke PB. Male circumcision decreases penile sensitivity as measured in a large cohort. BJU Int. 2013; 111: 820-827.
13. Kim D, Koo SA, Pang MG. Decline in male circumcision in South Korea. BMC Public Health. 2012; 12: 1067.