RESEARCH ARTICLE
Hippokratia 2016, 20(3):214-221
Vourli G1, Papatheodoridis G2, Raptopoulou M3, Dalekos GN4, Hounta A5, Nikolopoulou G6, Zouboulis-Vafeiadis I7, Manesis E8, Kitis G9, Gogos C10, Ketikoglou I11, Hatzis G12, Vasilialdis T13, Karatapanis S14, Mimidis K15, Drakoulis C16, Touloumi G1, The HEPNET-Greece study
1Department of Hygiene, Epidemiology and Medical Statistics, Athens University Medical School, Athens, 2Department of Gastroenterology, Athens University Medical School, “Laiko” General Hospital of Athens, Athens, 34th Medical Department, Aristotle University of Thessaloniki, Thessaloniki, 4Department of Medicine & Research Laboratory of Internal Medicine, School of Medicine, University of Thessaly, Larissa, 4th Department of Internal Medicine, General University Hospital “Attikon”, Athens, 6Viral Hepatitis Committee, KEELPNO, Athens, 7First Department of Propaedeutic Medicine, Athens University Medical School “Laiko” General Hospital of Athens, Athens, 8Division of Internal Medicine, Athens University Medical School, Athens, 9Gastroenterology Clinic, General Hospital “G. Papanikolaou”, Thessaloniki, 10Department of Infectious Diseases, Patras University Hospital, Patras, 11Department of Internal Medicine, “Hippocration” General Hospital, Athens, 12Department of Pathophysiology, University of Athens, Athens, 133rd Department of Internal Medicine, Aristotle University of Thessaloniki, “Papageorgiou” Hospital, Thessaloniki, 14Department of Internal Medicine, General Hospital of Rhodes, Rhodes, 15Department of Medicine, Democritus University of Thrace, Alexandroupolis, 162nd Department of Internal Medicine, General Hospital of Nikaia, Athens, Greece
![]()
Abstract
Background and Aims: Although effective treatment in terms of inducing virological and biochemical response for chronic hepatitis B (CHB) is available, its effect on the clinical course of the disease has not yet been accurately estimated. Objective of this study was to evaluate the effect of antiviral therapy and its type [interferon +/- nucleos(t)ide analogs (NAs) vs. NAs] on the occurrence of a clinical event (liver decompensation, liver transplant, hepatocellular carcinoma and death from a liver-related cause) in CHB patients.
Methods: The study population was derived from the HEPNET-Greece, a nationwide cohort study aimed to evaluate the current epidemiological course of viral hepatitis. To account for time-dependent confounding, Cox marginal structural models were used to analyze data.
Results: Thirty out of 2,125 eligible patients experienced a clinical event during their follow-up. When comparing treated to untreated individuals, the hazard ratio (HR) for a clinical event was 0.39 (95% CI: 0.16-0.98; p =0.044) in the whole sample, whereas there were indications of a more intense effect in the subgroup of patients with cirrhosis at presentation (HR =0.16, 95% CI: 0.02-1.21; p =0.075). The effect of Interferon initiated treatment was not significantly different of that of NAs. There was some evidence, albeit not statistically significant, of a protective treatment effect on hepatocellular carcinoma development (HCC).
Conclusions: Data from observational studies can provide useful inference, provided they are analyzed appropriately. The current study has shown that the available treatment options for CHB offer a significant clinical benefit to CHB infected individuals. Hippokratia 2016, 20(3): 214-221
Key words: Chronic Hepatitis B, survival, hepatocellular carcinoma, marginal structural models
Corresponding author: Georgia Vourli, Department of Hygiene, Epidemiology and Medical Statistics, Athens University Medical School, Mikras Asias 75, 11527 Goudi, Greece, fax: +302107462030, e-mail: gvourli@med.uoa.gr
Introduction
Chronic hepatitis B virus infection (CHB) remains a major public health issue. Although vaccine programs have decreased the incidence of hepatitis B virus (HBV)1, more than 350 million people are still infected with HBV worldwide2. CHB can lead to cirrhosis, hepatic decompensation, and hepatocellular carcinoma (HCC)1,3,4. It is estimated that approximately 780,000 people die every year due to CHB consequences5.
Current recommended treatment of CHB includes pegylated interferon alfa (PEG-IFNa) or one of the high genetic barrier- nucleos(t)ide analogs (NAs), entecavir or tenofovir, while standard interferon alfa (IFNa) or other NAs (lamivudine, adefovir, telbivudine) have also been used in the previous years6. Although the ultimate goal of antiviral therapy is to prevent disease progression and liver-related mortality, including HCC deaths, for practical reasons, the efficacy of antiviral therapy in almost all randomized controlled trials (RCTs) has been evaluated using surrogate end points such as virological (suppression of HBV replication) and/or biochemical [alanine transaminase/aspartate transaminase (ALT/AST) normalization] response7-13. Only one RCT had the power to evaluate treatment effects on long-term clinical events14. Whereas there is evidence that virological response is correlated with improved liver histology15-17, this does not necessarily imply equal antiviral effects on clinical relevant outcomes. Although RCTs provide the highest level of evidence, given the proven efficacy of current antivirals, a placebo-controlled trial would have been unethical, even in the context of a large multicenter RCT. Thus, such data have to come from observational studies.
Most previous studies and meta-analyses14,18,19 have found that antiviral therapy decreases liver-related, and all-cause mortality, but data on its effects on HCC development are less consistent20. Reliable estimates of antiviral effects across different geographical/ethnical groups are desirable for patients and their physicians, as well as, for public health planning and cost effectiveness calculations. When comparing different treatment groups, results from observational studies are known to be subject to biases due to treatment given by indication. Indeed, a recent meta-analysis20 has highlighted the essential role that research design plays on overall assessment and in particular in HCC incidence estimates.
Several methods have been proposed and implemented to avert induced biases including multivariable analysis, in which all known and measured confounders are included in the final model; propensity matching in which treated and untreated individuals are matched using propensity scores and inverse probability weighting (IPW) in which individuals are weighted proportionally to the inverse probability of treatment initiation. The pros and cons of each method have been previously discussed21,22. Although the least efficient, multivariable analyses approach is the most commonly used due to its simplicity. Propensity matching has been applied when analyzing data from CHB patients23. IPW, although commonly used when analyzing cohorts of HIV-infected individuals, to our knowledge, it has never been used in the analysis of cohorts of CHB infected individuals. Marginal structural models (MSMs), whose parameters are estimated using the IPW method, are particularly helpful for longitudinal cohort studies with time-varying confounders. In CHB cohorts, markers as ALT/AST or HBV DNA act as time-varying confounders, in the sense that they are risk factors for disease progression but also predict initiation of treatment, whereas they are subsequently affected by treatment. It is well established nowadays that in such situations inference using classic multivariable survival analysis techniques can be seriously biased24. To account for time-dependent confounding, we applied a Cox marginal structural model (MSM).
Therefore, our aim was to estimate the effect of antiviral treatment, as well as the effect of the type of treatment (IFNa initiated, NAs or none), on liver-related clinical events and particularly on HCC development, in CHB Caucasian patients. For that, we used data from a nationwide cohort study, the HEPNET-Greece.
Methods
Study population
The HEPNET-Greece network, aiming to evaluate the current epidemiological course of chronic HBV and hepatitis C virus, was established in 2003 with the support of the Hellenic Center for Disease Control and Prevention (HCDCP, KEELPNO, Greece). Twenty-five tertiary liver centers throughout Greece participate in the network. A structured case report form (CRF) was used for data collection. Before the network establishment, data were collected retrospectively from patients’ medical records and prospectively, updated twice per year, thereafter. Since 2005, written CRFs were replaced by electronic CRFs. All CRFs were submitted to the Statistical and Management Center based in the Department of Hygiene, Epidemiology and Medical Statistics, at the Medical School of Athens University. Extensive quality controls were performed to identify possible duplications, logical errors and missing or unexpected values. The study protocol was reviewed and approved by the Governing body of HCDCP.
All patients with CHB (HBsAg positivity for at least six months) were potentially eligible.
Patients who had visited a collaborating center before January 2000 were excluded from the sample since before this date NAs were not available in Greece. Baseline was defined as the first visit at which a biochemical exam was performed, the first HBV DNA was measured, or 1/1/2000, whichever latest. Patients were also excluded if they were co-infected with human immunodeficiency or hepatitis C or D viruses; were ≤16 years old at baseline; had previous treatment or were on treatment at baseline; had experienced a liver-related event before or within one month after the baseline visit or had been followed for less than one month.
Definitions
The diagnosis of cirrhosis was based on histological findings (Ishak’s stage 5 or 6)25 or, in patients without a liver biopsy, on previously described physical examination, endoscopic and/or ultrasonographic findings26,27.
Treatment was categorized into two groups: IFNa initiated therapy (IFNa group), which included (PEG-)IFNa monotherapy or (PEG-)IFNa with subsequent NA therapy, and NA therapy alone (NA group). All analyses were conducted on an ‘intention-to-treat’ basis, that is, the decision to treat was actually evaluated. Thus, patients were considered as treated irrespectively of the treatment duration.
A clinical event was defined as one of the following: liver decompensation (variceal bleeding, ascites, hepatic encephalopathy), HCC, liver transplant or liver-related death. Date of an event was considered as the date of the earliest of the above-mentioned events. Follow-up was the time interval between baseline visit and date of clinical event development, date of last clinical assessment or August 2012 whichever came first. To estimate the effect of treatment on the time to HCC development, HCC was considered as the only relevant event, while patients who did not experience HCC were censored at the date they were last seen alive.
Statistical analysis
In order to estimate the average hazard ratio (HR) for CHB treatment initiation versus noninitiation, as well as for the type of CHB treatment initiation, i.e., IFNa initiated or NA alone versus no treatment initiation, two pooled logistic models were fitted. Both models included a time-varying indicator for ever use of treatment (or the type of treatment), time of follow-up in months as restricted cubic splines with 5 knots and a set of baseline covariates: ALT (≤40 IU/L, >40 IU/L), AST (≤40 IU/L, >40 IU/L) HBV DNA level (≤2000 IU/mL, >2000IU/mL), cirrhosis, sex, age, calendar year, years since HBV diagnosis. In all cases, the baseline status was considered as the patient’s status at baseline or within one month window from the start of follow-up.
The data analyzed in the current study come from an observational study where patients are treated by indication; therefore treatment’s effect is subject to confounding. Standard methods propose adjustment by including covariates in multivariable models. It has been shown though that in cases where i) a time-dependent covariate exists (e.g. a biochemical marker such as ALT) that is both a risk factor for clinical disease progression and also predicts subsequent exposure and ii) past exposure history predicts the risk factor, this approach may lead to biased estimates.
To avoid such bias, we used a Cox MSM to estimate the treatment’s effect28. Treatment was considered as either a binary covariate (treated/untreated) or a multinomial covariate with three levels (IFNa group/NA group/untreated). In a preliminary step, stabilized treatment weights were constructed according to the Inverse Probability of Treatment Weighting (IPTW) method.
Following the above described procedure, we intended to mimic a trial, where patients initiate treatment randomly at each time point. Assuming that all time-dependent confounders are available for the analysis, the effect of treatment was estimated unbiasedly.
Each patient was assigned a time-updated weight, which was inversely proportional to the probability of having his/her own observed history of treatment initiation, as this was estimated by either the logistic regression or the multinomial models28,29. To estimate each patient’s probability of treatment initiation in each month, we fit a pooled logistic model that included time-varying covariates for ALT, AST, HBV DNA, cirrhosis, along with age and sex, and an indicator for an interval greater than three months since last lab measure. Variables’ selection for both models, i.e., the treatment and the survival model, was performed following recommendations by Moodie30.
The mean of the estimated weights was 1.15 (1st percentile: 0.05, 99th percentile: 5.63) in the case of binary treatment and 1.09 (1st percentile: 0.01, 99th percentile: 5.43) in the case of multinomial treatment (i.e., type of treatment). Since their range was acceptable and their mean did not substantially deviate from 1, no weights truncation was applied.
The pooled logistic regression accounts for the within-subject correlation thus 95% confidence intervals (CI) were computed by using robust variance estimators.
In order to separately estimate the average treatment effect in patients with different disease severity, subset analysis according to the baseline cirrhosis status was performed.
Two sensitivity analyses were performed: Artificial censoring a) at the first time patient was not seen for 18 months or more, or b) at the time a patient initiated a new treatment. In all analyses, censoring weights were estimated and incorporated in the final model. The analysis was repeated for the overall clinical disease progression, i.e. considering death from any cause as an event. Moreover, the analysis was repeated in the subgroup of hepatitis B e antigen (HBeAg) negative at baseline patients.
Cox MSMs were fitted by pooled logistic regression using the Stata 11.2 software (StataCorp, College Station, Texas USA), as described previously31. For comparison, treatment’s effect was estimated by standard (unweighted) Cox models, unadjusted and adjusted for all significant time-dependent covariates or their baseline values.
Results
Up to August 2012, 6,921 CHB patients were enrolled in the HEPNET-Greece study, of which 6,238 were mono-infected adults. Of them, 4,960 first visited a collaborating center after 2000, 3,670 had at least one ALT and one HBV DNA measurement, whereas 2,125 were followed for at least one month, treatment naïve and event free at baseline (and for the first month of follow-up). Details on the baseline status of the 2,125 eligible patients are shown in Table 1.
Patients were followed for a median time of 28 months [interquartile range (IQR) 12-57 months]. During follow-up, 679 (32%) patients initiated treatment. Specifically, 319 of them were initially treated with IFNa, either alone (n =248) or in combination with NA (n =71), while 360 patients were treated only with NA(s) (Table 2). Two hundred and fifty-one of the 360 NA-treated (69.7%) received lamivudine and/or adefovir. Overall, 30 (1.4%) patients experienced a clinical event in 4-100 months from baseline. Eleven of these events (36.7%) were observed in patients who had not been treated yet (six cases of decompensated cirrhoses, four of HCC and one liver-related death), seven (23.3%) in patients who had received IFN-IFNa based treatment (two cases of decompensated cirrhosis and five of HCC) and 12 events (40.0%) in patients who had received NAs (four cases of decompensated cirrhosis, eight of HCC). Eight (47.1%) of the patients that developed HCC had not a prior cirrhosis diagnosis.
Patients with cirrhosis (OR: 1.56, 95% CI: 1.15-2.11; p =0.004), HBV DNA >2000 IU/ml (OR: 8.52, 95% CI: 6.5-11.23; p <0.001), and elevated ALT (OR: 4.75, 95% CI: 3.78, 5.96; p <0.001) or AST (>40 IU/L) (OR: 2.59, 95% CI: 2.13-3.15; p <0.001) were more likely to initiate treatment. Factors affecting the probability of starting IFNa based treatment also had a similar effect on the probability of starting an NA based regimen. Patients with cirrhosis though were more likely to initiate treatment with NAs [Relative Risk Ratio (RRR): 1.50, 95% CI: 0.90-2.50; p =0.116 for IFNa initiation and RRR: 1.98, 95% CI: 1.38-2.85; p <0.001]. Elevated HBV DNA was a stronger prognostic factor for initiating IFNa than NA treatment (RRR: 18.10, 95% CI: 9.58-34.21; p <0.001 for IFNa initiation and RRR: 7.01, 95% CI: 4.95-9.93; p <0.001). Older patients were more likely to be treated with NAs, whereas younger were more likely to be treated with IFNa (RRR for one year of age: 1.03, 95% CI: 1.02-1.04; p <0.001 for NAs and RRR for one year of age: 0.99, 95% CI: 0.98-0.99; p <0.001 for IFNa). In addition, women tended to be more likely to initiate NA treatment (RRR for NAs initiation 1.23, 95% CI: 0.98-1.53, p =0.075).
According to the MSM Cox model, treatment was found to reduce the hazard of a clinical event by about 60% (HR =0.39, 95% CI: 0.16-0.98; p =0.044). The effect of treatment was found to be more intense in the subgroup of patients with cirrhosis than in the subgroup of cirrhosis-free at baseline patients, although results were not statistically significant for either group (HR =0.16, 95% CI: 0.02-1.21; p =0.075 and HR =0.45, 95% CI: 0.10-2.05; p =0.300, respectively) (Table 3). When the effect of treatment type was assessed, the results were in the same direction, implying a protective though non-significant effect of both IFNa and NA treatment. Specifically, IFNa was found to decrease the hazard by almost 65% compared to no treatment (HR =0.36, 95% CI: 0.10-1.31; p =0.122), while treatment with NAs was also protective (HR =0.45, 95% CI: 0.18-1.12; p =0.093). The analysis of the overall mortality, i.e. considering six deaths from non-liver causes as events, as well as the analysis that was restricted to HBeAg negative at baseline patients, gave similar results (data not shown).
Analysis revealed that treatment is protective against HCC as well, although this finding failed to reach statistical significance (HR =0.54, 95% CI: 0.16-1.79; p =0.313). The effect of IFNa was found identical to that of NAs (HR =0.55, 95% CI: 0.13-2.36; p =0.419 and HR =0.55, 95% CI: 0.16-1.91; p =0.346 for IFNa and NA versus no treatment, respectively).
Of the 679 treated patients, 274 received a new regimen directly after stopping the first one or at a later stage. Artificial censoring the follow-up at the time of second treatment initiation and repeating the analysis with appropriate adjustments (through inverse probability of censoring weighting) resulted in similar estimates of the treatment and the treatment type effects. However, probably due to the fact that ten events were censored, results in this case were not significant.
ALT and AST were measured for a median of five times (IQR 2-9 times), with a median interval between these measurements of 5.7 months (IQR 3-9 months).
The median number of available measurements of HBV DNA was two (IQR 1-5), with a median interval between these measurements of 8 months (IQR 5.4 -13 months).
To account for potential bias due to infrequent follow-up, data were artificially censored at the first time an interval of more than 18 months without a biochemical exam was recorded. Repeating the analysis incorporating appropriate adjustments as described before yielded results similar to those of the main analysis (data not shown).
Analysis Ignoring Time Dependent Confounding
In a univariable Cox regression analysis, treatment seemed to double the hazard of an event (HR =2.30, 95% CI: 1.11-4.76; p =0.025). This was mainly due to NA as treatment with NA appeared to be significantly associated with three times the hazard of the untreated (HR =2.80, 95% CI: 1.28-6.11; p =0.010) whereas treatment with IFNa appeared to have still harmful but smaller and non-significant effect (HR =1.76, 95% CI: 0.67-4.65; p =0.250).
When adjusting for time-dependent confounders (gender, age, presence of cirrhosis, elevated ALT/AST, calendar year and HBV DNA), treatment was not found to have a protective effect achieving a non-significant hazard reduction of 7% (HR =0.93, 95% CI: 0.35-2.41; p =0.874). Similarly, the effect of both IFNa and NA versus no treatment were very close to the overall treatment effect, reducing the hazard by 6% and 21%, respectively (HR =0.94, 95% CI: 0.31-2.88; p =0.918 for IFN, and HR =0.79, 95% CI: 0.29-2.11); p =0.633 for the NAs).
Adjusting for baseline values only, the protective effect of treatment was similar to that estimated after adjusting for time-dependent confounding (HR =0.81, 95% CI: 0.30-2.23; p =0.688). However, in this case, the effect of both treatment approaches was more apparent (IFNa vs. no treatment: HR =0.77, 95% CI: 0.22-2.71; p =0.679 and NA vs. no treatment: HR =0.65, 95% CI: 0.23-1.86; p =0.427).
The comparison of the different modeling approaches, the estimated effects of treatment and type of treatment from all the applied methods, are shown in Figure 1.
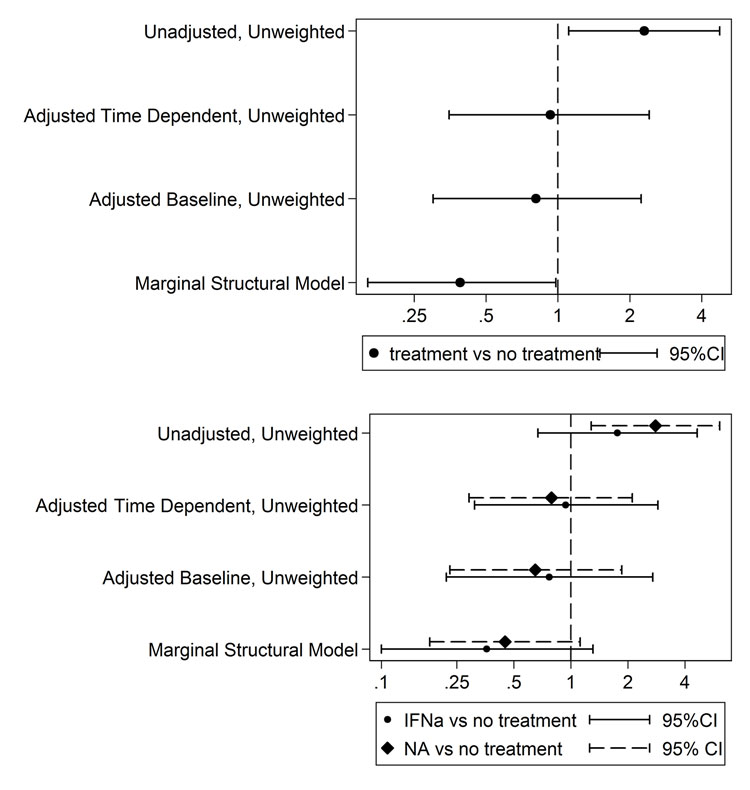
Figure 1: Estimated effect of treatment (upper plot) and the type of treatment (lower plot), from unweighted (standard) unadjusted, adjusted by baseline covariates only and adjusted by time dependent covariates and weighted Cox models.
Discussion
Our results showed that the hazard of a clinical event, i.e., liver decompensation, liver transplant, HCC or death from a liver-related cause, is significantly reduced by 60% (p =0.044) in treated patients compared to untreated peers. This effect was much more intense in the subgroup of patients with cirrhosis at study entry, although not statistically significant at the nominal significance level, due to the smaller number of events included in this subanalysis (p =0.075). Both IFNa-initiated and NA therapy seem to offer a similar benefit. Compared to no treatment, the hazard of a clinical event was reduced by 65% (p =0.122) and 55% (p =0.093) by IFNa-initiated and NA treatment, respectively. Moreover, our results indicate that both NA and IFNa-initiated therapy are equally protective against HCC, albeit this finding was not found to be statistically significant, presumably due to low statistical power. Our finding of 60% reduction of the hazard of a clinical event in treated compared to untreated CHB patients is consistent with previously reported results14,18,19.
A meta-analysis of non-comparative, observational studies has indicated that treatment with lamivudine and telbivudine significantly decreased clinical disease progression and disease severity32. Moreover, HBsAg clearance can occur in CHB patients treated with lamivudine, achieving this way a protective effect against clinical progression33.
Early clinical trials comparing active treatment (mainly IFNa courses or lamivudine initiated) to placebo provided encouraging results in terms of virologic or biochemical response11,34-36. Concerning the type of treatment, results from a non-randomized historic control study have shown that lamivudine significantly reduces the hazard of a clinical event by 40% compared to untreated and by 55% compared to IFN treated non-sustained responders37. In that study though, there was a significant difference in clinical events between IFNa treated and untreated patients, but IFNa baseline characteristics differed between the two groups.
Newer NAs appear to be significantly superior to lamivudine in terms of virologic response and ALT normalization, for both HBeAg positive and negative patients9,10,12,38,39. These surrogate markers have been recognized as effective measures of response to treatment15. However, results based on surrogate markers are not necessarily translated to equivalent results on clinical outcomes. Since findings from early treatment versus placebo trials suggest that treatment is indeed protective14, trials that include a placebo arm can no longer be performed. Thus, direct evidence of antiviral therapy on long-term disease progression and/or liver-related mortality can only be obtained from appropriately analyzed observational studies. We believe that presented results contribute valuable information, as our analysis mimics a randomized clinical trial. In the current study, we found a similar protective effect on clinical events of both strategies, starting with NAs or IFNa.
Reducing the risk of HCC is one of the most important milestones of treatment40. Results regarding IFNa effect on reducing HCC are controversial41. Recently published studies in which the effect of NAs treatment on the risk of HCC was assessed, have found a significant or at least marginally significant protective effect14,23,42. Nevertheless, there are only a few studies on this issue in Caucasians, and overall results are inconclusive20. We found that both IFNa initiated and NA therapies reduce by about 45% the hazard of HCC. However, our study was underpowered to detect these effects at a significant level.
Observational studies with survival endpoints usually suffer from drawbacks that can severely affect the estimation of the effects of treatments. One such drawback, that usually occurs, is selection bias. In the case, for example, of including patients at treatment initiation, the subgroup of patients that had survived or were followed long enough to initiate treatment, are included in the study. This could result in a study population that is not representative of the whole population of CHB patients. Another issue that always interferes with inference, especially in studies that include historic controls, is that it is difficult if not impossible to account and/or adjust for differences in the calendar period in which each treatment was given. To overcome the problem of non-comparability of patients treated in different time periods, we excluded patients that had visited a collaborating center earlier than January 2000, when lamivudine became available in Greece. Moreover, the baseline calendar year was included in the treatment model, to make groups comparable with respect to when they were treated.
In all cases, weighted Cox models gave more intense estimates of treatments effect compared to those obtained through traditional analyses (i.e., through univariable or multivariable unweighted Cox models). This result is due to the bias induced by the standard analysis techniques when time-dependent confounding (i.e., confounding by indication) is present43. MSM Cox models adjust for confounding through weighting and not by including time-dependent confounders in the survival model. Confounding by indication makes even more problematic an analysis whose interest lies on differentiating the effect of the two treatment approaches (IFNa and NA), than when the overall treatment’s effect is the main goal.
Weights estimation in the preliminary step of the MSM Cox models we used, rely on the correct modeling of the probability of treatment initiation. Explicitly, this means that we need full information on all parameters that affect the decision to initiate treatment. Given that the major treatment confounders (i.e. ALT, AST, and HBV DNA) are relatively frequently available, and that patients’ liver cirrhosis status is known, this was a reasonable assumption in the current study.
As mentioned in previous studies that applied weighted Cox models to HIV patients, it is important to notice that we mimic a trial where patients are randomly allocated to treatment (or type of treatment) at baseline; thus our estimates correspond to intention-to-treat estimates44,45. This means that our estimates correspond to the effect of treatment had all patients been treated from the start and throughout their follow-up. Alternatively, the efficacy of treatments could be assessed after restricting the analysis to those with virological response only. Results of such analyses can be interpreted conditional on patients’ response and thus cannot be generalized to inference for treatment choices at presentation. Effect estimates from such analyses are expected to be more intense compared to our estimates which refer to the average effect of treatment, irrespectively of any intermediate treatment goals achieved.
In the current study, only baseline eligibility criteria were applied. Thus, probably some inactive CHB patients, who would not experience a clinical event even if had been left untreated, were included. These patients have a high probability of remaining untreated given their characteristics (absence of cirrhosis, low ALT/AST, and HBV DNA levels). If they were actually left untreated as expected, they would receive a low weight in our analysis. On the other hand, if they were treated despite their covariate pattern, they would have a very large weight. Thus, potential confounding is taken into account through weighting, in this case, too. It must be pointed out that we had no indication of potential influential records since the weights used in our analysis had no extreme values. A sensitivity analysis in the subgroup of patients with ALT >40 IU/L gave results in the same direction with our main analysis results (i.e. protective treatment effect and similar effects for both treatment strategies), though non-statistically significant due to the subsequent loss of power. Therefore, disease inactivity seems to be adequately taken into account in our analysis.
Due to the constraints and the practical difficulties of running clinical trials with survival endpoints in patients with CHB, data from observational studies will continue to provide us with valuable information. However, as we discussed above, observational studies are subject to serious bias when comparing treatment groups, due to lack of randomization. Thus, particular attention should be paid to apply appropriate analysis to take into account time-dependent confounding that often occurs. Although the propensity score matching offers an alternative, it has been previously documented it only accounts for baseline confounding22. In this study we displayed how the method of MSM could be used when analyzing observational data. We believe that this is a powerful method that should be used more often when the aim is to compare different treatment groups using observational cohort studies’ data. Most importantly, large cohorts and international collaborations are needed in order to have enough statistical power to assess the effect of newer anti-viral agents and distinguish between them.
To conclude, presented results suggest that therapy decreases the risk of a clinical event by 60% in the total population of CHB patients. Both NA and IFNa initiated treatment may offer a prophylactic effect; however we failed to differentiate their effects. A limitation of our study is that a large proportion of NA treated patients received lamivudine or adefovir based schemes. Only 30% of the NA treated patients were originally treated with newer agents, such as tenofovir and entecavir. Since newer agents are more effective than lamivudine, our results possibly underestimate the overall treatment effect. Moreover, 22% of the patients treated with IFNa based regimens received a NA, mainly lamivudine, along with IFNa. Grouping these patients together with those on IFNa monotherapy may have diluted any difference in survival between IFNa and NA effect of treatment. Regarding HCC, results from recent, large studies are controversial, therefore further research on this topic is essential20.
Conflict of interest
Authors report no conflict of interest.
References
1. Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012; 30: 2212-2219.
2. Liaw YF, Chu CM. Hepatitis B virus infection. Lancet. 2009; 373: 582-592.
3. Ly KN, Xing J, Klevens RM, Jiles RB, Ward JW, Holmberg SD. The increasing burden of mortality from viral hepatitis in the United States between 1999 and 2007. Ann Intern Med. 2012; 156: 271-278.
4. El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011; 365: 1118-1127.
5. World Health Organization. Hepatitis B. Fact sheet N°204. Available at: http://www.who.int/mediacentre/factsheets/fs204/en/, last accessed on 01/05/2016.
6. European Association For The Study Of The Liver. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol. 2011; 57: 167-185.
7. Marcellin P, Chang TT, Lim SG, Tong MJ, Sievert W, Shiffman ML, et al; Adefovir Dipivoxil 437 Study Group. Adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. N Engl J Med. 2003; 348: 808-816.
8. Marcellin P, Lau GK, Bonino F, Farci P, Hadziyannis S, Jin R, et al; Peginterferon Alfa-2a HBeAg-Negative Chronic Hepatitis B Study Group. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med. 2004; 351: 1206-1217.
9. Marcellin P, Heathcote EJ, Buti M, Gane E, de Man RA, Krastev Z, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med. 2008; 359: 2442-2455.
10. Lai CL, Shouval D, Lok AS, Chang TT, Cheinquer H, Goodman Z, et al; BEHoLD AI463027 Study Group. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med. 2006; 354: 1011-1020.
11. Dienstag JL, Schiff ER, Wright TL, Perrillo RP, Hann HW, Goodman Z, et al. Lamivudine as initial treatment for chronic hepatitis B in the United States. N Engl J Med. 1999; 341: 1256-1263.
12. Chang TT, Gish RG, de Man R, Gadano A, Sollano J, Chao YC, et al; BEHoLD AI463022 Study Group. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med 2006; 354: 1001-1010.
13. Janssen WJ, Collard HR, Saint S, Weinberger SE. Clinical problem-solving. A perfect storm. N Engl J Med. 2005; 353: 1956-1961.
14. Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, et al; Cirrhosis Asian Lamivudine Multicentre Study Group. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004; 351: 1521-1531.
15. Aghemo A, Lampertico P, Colombo M. Assessing long-term treatment efficacy in chronic hepatitis B and C: between evidence and common sense. J Hepatol. 2012; 57: 1326-1335.
16. Chen CJ, Yang HI, Iloeje UH; REVEAL-HBV Study Group. Hepatitis B virus DNA levels and outcomes in chronic hepatitis B. Hepatology. 2009; 49: S72-S84.
17. Liaw YF. Hepatitis B virus replication and liver disease progression: the impact of antiviral therapy. Antivir Ther. 2006; 11: 669-679.
18. Wong GL, Yiu KK, Wong VW, Tsoi KK, Chan HL. Meta-analysis: reduction in hepatic events following interferon-alfa therapy of chronic hepatitis B. Aliment Pharmacol Ther. 2010; 32: 1059-1068.
19. Manolakopoulos S, Karatapanis S, Elefsiniotis J, Mathou N, Vlachogiannakos J, Iliadou E, et al. Clinical course of lamivudine monotherapy in patients with decompensated cirrhosis due to HBeAg negative chronic HBV infection. Am J Gastroenterol. 2004; 99: 57-63.
20. Thiele M, Gluud LL, Dahl EK, Krag A. Antiviral therapy for prevention of hepatocellular carcinoma and mortality in chronic hepatitis B: systematic review and meta-analysis. BMJ open. 2013; 3: pii: e003265.
21. Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav Res. 2011; 46: 399-424.
22. Kurth T, Walker AM, Glynn RJ, Chan KA, Gaziano JM, Berger K, et al. Results of multivariable logistic regression, propensity matching, propensity adjustment, and propensity-based weighting under conditions of nonuniform effect. Am J Epidemiol. 2006; 163: 262-270.
23. Lim YS, Han S, Heo NY, Shim JH, Lee HC, Suh DJ. Mortality, liver transplantation, and hepatocellular carcinoma among patients with chronic hepatitis B treated with entecavir vs lamivudine. Gastroenterology. 2014; 147: 152-161.
24. Robins JM, Hernán MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000; 11: 550-560.
25. Ishak K, Baptista A, Bianchi L, Callea F, De Groote J, Gudat F, et al. Histological grading and staging of chronic hepatitis. J Hepatol. 1995; 22: 696-699.
26. Colli A, Fraquelli M, Andreoletti M, Marino B, Zuccoli E, Conte D. Severe liver fibrosis or cirrhosis: accuracy of US for detection–analysis of 300 cases. Radiology. 2003; 227: 89-94.
27. Manesis EK, Papatheodoridis GV, Touloumi G, Karafoulidou A, Ketikoglou J, Kitis GE, et al. Natural course of treated and untreated chronic HCV infection: results of the nationwide Hepnet.Greece cohort study. Aliment Pharmacol Ther. 2009; 29: 1121-1130.
28. Hernán MA, Brumback B, Robins JM. Marginal structural models to estimate the causal effect of zidovudine on the survival of HIV-positive men. Epidemiology. 2000; 11: 561-570.
29. Robins JM. Non-response models for the analysis of non-monotone non-ignorable missing data. Stat Med. 1997; 16: 21-37.
30. Moodie EE. Risk factor adjustment in marginal structural model estimation of optimal treatment regimes. Biom J. 2009; 51: 774-788.
31. Fewell Z, Hernan M. Controlling for time-dependent confounding using marginal structural models. Stata J. 2004; 4: 402.
32. Huang Y, Wu H, Wu S, Fu D, Ma Y, Shen X. A meta-analysis of nucleos(t)ide analogues in patients with decompensated cirrhosis due to hepatitis B. Dig Dis Sci. 2013; 58: 815-823.
33. Idilman R, Cinar K, Seven G, Bozkus Y, Elhan A, Bozdayi M, et al. Hepatitis B surface antigen seroconversion is associated with favourable long-term clinical outcomes during lamivudine treatment in HBeAg-negative chronic hepatitis B patients. J Viral Hepat. 2012; 19: 220-226.
34. Krogsgaard K. The long-term effect of treatment with interferon-alpha 2a in chronic hepatitis B. The Long-Term Follow-up Investigator Group. The European Study Group on Viral Hepatitis (EUROHEP). Executive Team on Anti-Viral Treatment. J Viral Hepat. 1998; 5: 389-397.
35. Mazzella G, Saracco G, Festi D, Rosina F, Marchetto S, Jaboli F, et al. Long-term results with interferon therapy in chronic type B hepatitis: a prospective randomized trial. Am J Gastroenterol. 1999; 94: 2246-2250.
36. Waked I, Amin M, Abd el Fattah S, Osman LM, Sabbour MS. Experience with interferon in chronic hepatitis B in Egypt. J Chemother. 1990; 2: 310-318.
37. Papatheodoridis GV, Dimou E, Dimakopoulos K, Manolakopoulos S, Rapti I, Kitis G, et al. Outcome of hepatitis B e antigen-negative chronic hepatitis B on long-term nucleos(t)ide analog therapy starting with lamivudine. Hepatology. 2005; 42: 121-129.
38. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, Chang TT, Kitis G, Rizzetto M, et al; Adefovir Dipivoxil 438 Study Group. Adefovir dipivoxil for the treatment of hepatitis B e antigen-negative chronic hepatitis B. N Engl J Med. 2003; 348: 800-807.
39. Lai CL, Gane E, Liaw YF, Hsu CW, Thongsawat S, Wang Y, et al; Globe Study Group. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med. 2007; 357: 2576-2588.
40. Janssen HL, Arif A. Averting hepatocellular carcinoma in chronic hepatitis B with antiviral therapy: tipping the balance or not yet? Gastroenterology. 2014; 147: 24-26.
41. Seo Y, Yano Y. Short- and long-term outcome of interferon therapy for chronic hepatitis B infection. World J Gastroenterol. 2014; 20: 13284-13292.
42. Wu CY, Lin JT, Ho HJ, Su CW, Lee TY, Wang SY, et al. Association of nucleos(t)ide analogue therapy with reduced risk of hepatocellular carcinoma in patients with chronic hepatitis B: a nationwide cohort study. Gastroenterology. 2014; 147: 143-151.e5.
43. HIV-CAUSAL Collaboration, Ray M, Logan R, Sterne JA, Hernández-Díaz S, Robins JM, et al. The effect of combined antiretroviral therapy on the overall mortality of HIV-infected individuals. AIDS. 2010; 24: 123-137.
44. Sterne JA, Hernán MA, Ledergerber B, Tilling K, Weber R, Sendi P, et al. Long-term effectiveness of potent antiretroviral therapy in preventing AIDS and death: a prospective cohort study. Lancet. 2005; 366: 378-384.
45. Cole SR, Hernán MA, Robins JM, Anastos K, Chmiel J, Detels R, et al. Effect of highly active antiretroviral therapy on time to acquired immunodeficiency syndrome or death using marginal structural models. Am J Epidemiol. 2003; 158: 687-694.