CASE REPORT
Hippokratia 2017, 21, 1: 46-48
Krzyżanowski A1, Kwiatek M1, Gęca T1, Barczyński B2, Kwaśniewska A1
1Department of Obstetrics and Pathology of Pregnancy, 2Department of Oncological Gynecology and Gynecology, Medical University of Lublin, Poland
![]()
Abstract
Background: Amniotic band syndrome (ABS)is a rare disorder which leads to a number of deformities of the fetus body. The treatment depends on the severity of the defect and the extent of the deformity. Case report: A 36-year-old primigravida with a dichorionic diamniotic (DCDA) twin pregnancy was diagnosed during the first-trimester ultrasonography with fetal lower part edema of one twin caused by amniotic bands. A selective termination of the affected fetus was performed. The remainder part of the pregnancy was normal. A healthy newborn was delivered at term. After delivering the placenta, the presence of fetus papyraceus was detected. The amniotic bands were unidentifiable in the pathologist’s examination. A reliable ultrasonographic diagnosis enables the detecting ABS in early pregnancy. Conclusion: In the case of ABS in DCDA twin pregnancy, conducting a selective termination of the affected fetus creates the opportunity for the proper development of the healthy fetus as well as reaching its full maturity. HIPPOKRATIA 2017, 21(1): 46-48.
Key words: Amniotic band syndrome,dichorionic diamniotic twin pregnancy, selective termination
Corresponding author: Maciej Kwiatek, Department of Obstetrics and Pathology of Pregnancy, Medical University of Lublin, Poland, tel/fax: +48815326612, e-mail: kwiatula1@wp.pl
Introduction
Amniotic band syndrome (ABS) occurs with a frequency ranging from 1 in 1,200 to 1 in 15,000 live births1. Its incidence in multiple pregnancies seems to be very low and has never been precisely determined. The clinical manifestation of ABS depends on the location of the constricting amniotic bands, as well as on the severity of their constriction on the fetus. Bands surrounding vital areas, such as the umbilical cord or the head, are the most life-threatening. The defects caused by amniotic bands are usually asymmetric and polymorphic. The most common clinical symptoms of ABS are deformities of the fingers and toes, including their amputation. Rings constricting other body parts, causing injuries to the chest and abdominal wall, are observed more rarely2. If limb defects coexist with other severe deformations, including anterior body wall defects and/or exencephaly with facial clefts, such a polymalformation is called limb-body wall complex (LBWC)3. However, some studies tend to distinguish these two entities – LBWC and ABS – on exclusively epidemiologic grounds4,5.
We report here on a case of ABS diagnosed in the first trimester, selectively affecting one fetus in a dichorionic diamniotic (DCDA) twin pregnancy after in vitro fertilization (IVF). To the best of our knowledge, the case described is the first in which a selective termination was performed because of ABS and the gestation was completed with the delivery of a healthy newborn at term.
Case report
A 36-year-old primigravida with a DCDA twin pregnancy was diagnosed with fetal lower part edema of one twin during the first trimester (Figure 1A, 1B). The patient had been treated for infertility connected with ovulation disturbances and male factor. The pregnancy resulted from IVF. The pregnant woman was sent to the tertiary care center on the eleventh week of pregnancy to have an ultrasound (US) consultation conducted. The US scans revealed the presence of a constricting ring around the navel region of one twin that caused the aforementioned edema. A 3-dimensional (3-D) US confirmed the malformation. Amniotic band syndrome was diagnosed. At the same time, the first-trimester screening test (US scans + double test) for chromosomal abnormalities was performed. The risk of trisomy 21 was below 1:1700, whereas for trisomy 13/18 was less than 1:4500 for both fetuses. The patient was given three options: i) the selective termination (ST) of the compromised fetus, ii) the fetoscopic release of the amniotic bands, and iii) expectant management. On the 14th week of pregnancy, the pregnant woman decided to proceed to ST of the anomalous fetus, which was performed by an intra-cardiac injection of potassium chloride, without any further complications. The remainder part of the pregnancy was normal. At the 41st week of pregnancy, due to no progress of labor after the rupture of the amniotic sac, a cesarean section was performed. The delivered newborn baby girl weighed 3,240 grams with an APGAR of 10/10/10/10 measured in the 1st, 3rd, 5th, and 10th minute of life. After delivering the placenta, the presence of fetus papyraceus was detected, and was described by the pathologist as a compressed, completely macerated, fetus, presented as a yellowish-pink flaccid mass of an irregular shape, measuring 4.5 x 5.3 x 2.8 cm. The amniotic band was unidentifiable. In the microscopic examination, the structure of the fetal tissues was entirely effaced due to advanced autolytic changes (Figure 1C). The mother and the baby were discharged from hospital in good health, four days after delivery.

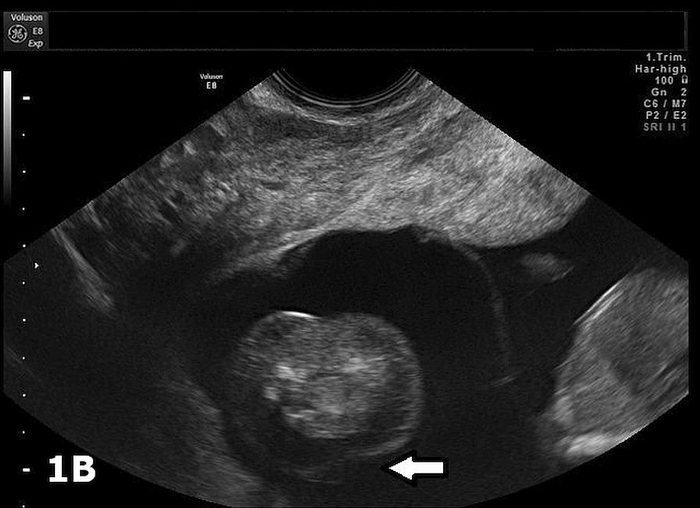

Figure 1: Longitudinal section (A) and cross section (B) ultrasound scan showing lower part edema of one twin during the first-trimester ultrasonographic scan of a dichorionic diamniotic (DCDA) twin pregnancy; (C) Compressed, macerated second fetus after delivery with no signs of amniotic bands.
Discussion
In the majority of cases, the diagnosis of amniotic bands is possible by the US, which has been already performed in the first trimester of pregnancy, or at the beginning of the second. While the revealing of amniotic bands is helpful, it does not lead, however, to the detection of ABS. 3D ultrasonography may improve the detection of facial and distal limb deformities6. Fetal lower part edema requires differentiation from fetal ascites, an early manifestation of nonimmune fetal hydrops, urinary ascites, and chyloperitoneum7. The discovery of amniotic bands presence during ultrasonography requires particular attention being paid to the fetus until the end of the pregnancy. ABS increases the risk of complications, which are dangerous for the fetus, including preterm delivery, low birth weight, and stillbirth5.
In order to prevent fetal limb amputation and/or intrauterine death, attempts are made to perform intrauterine surgeries. In each case, the parents must be thoroughly informed about the risk of such surgical intervention which in ABS involves the cutting of the amniotic bands by means of fetoscopy8. Another therapeutic method involves using a laser to reduce adhesions9. These treatments carry the risk of complications, such as rupture of the amniotic sac, or premature delivery10. The management in a multiple-gestation may be similar; however, the risk of complications after fetoscopy or laser therapy in a twin pregnancy seems to be much higher. Moreover, ethical and clinical dilemmas may arise when considering ABS treatment in a multiple-gestation.
ST in a multiple-gestation may be complicated by fetal loss and preterm delivery. The most frequent indications for such a procedure are chromosomal and structural abnormalities. In general, in twins, the risk of congenital defects and aneuploidy is increased in comparison to singletons11. We have not found any previous study concerning selective ABS in a twin pregnancy as an indication for ST. In our pregnant, the calculated risk for trisomy 13, 18, 21 was low for both fetuses, and the constricting amniotic band with edema of the lower part of one fetal body were the only abnormal findings.
The risk of fetal loss after ST may depend on the gestational age when the procedure is performed. There are studies which suggest that ST before 18 weeks of gestation is associated with a slightly lower loss rate12. However, other authors have found an equal loss rate in DCDA twins selectively terminated before and after the 20th week of gestation13, or an even higher loss rate when the procedure was carried out in the first half of the pregnancy14. None of the above studies proved a statistically significant correlation. The studies mentioned above gave similarly conflicting results with regard to the risk of a premature delivery.
The most recent study by Bigelow et al, conducted in a group of 80 patients who underwent ST before (n =47) and after (n =33) the 18th week of gestation showed that when the procedure was performed earlier it was not followed by any fetal loss, while in the group after the 18th week, a miscarriage occurred in four cases15. In women who delivered at term, the median gestational age at the time of ST was 14.1 weeks. In the group of preterm births after ST, the median gestational age at the time of ST was 18.7 weeks. The gestational age at the time of ST was the only characteristic independently associated with the risk of preterm delivery.
Our pregnant patient underwent ST in the 14th week of her twin pregnancy and delivered a healthy newborn at term. According to the pathologist’s description of the macerated second fetus after delivery, the amniotic bands were unidentifiable. In the case of ABS in a DCDA twin pregnancy, conducting the ST of the affected fetus creates an opportunity for the proper development of a healthy fetus as well as its reaching full maturity. Invasive methods of treatment seem to carry an unacceptably high risk for both fetuses in a DCDA twin pregnancy. With no therapeutic options for ABS in a multiple-pregnancy, an early ST carried out before the 18th week of gestation allows for the successful development of the other twin.
Conflict of interest
Authors declare no conflict of interest.
References
1. Cignini P, Giorlandino C, Padula F, Dugo N, Cafà EV, Spata A. Epidemiology and risk factors of amniotic band syndrome, or ADAM sequence. J Prenat Med. 2012; 6: 59-63.
2. Higginbottom MC, Jones KL, Hall BD, Smith DW. The amniotic band disruption complex: timing of amniotic rupture and variable spectra of consequent defects. J Pediatr. 1979; 95: 544-549.
3. Van Allen MI, Curry C, Gallagher L. Limb body wall complex: I. Pathogenesis. Am J Med Genet. 1987; 28: 529-548.
4. Guzmán-Huerta ME, Muro-Barragán SA, Acevedo-Gallegos S, Velázquez-Torres B, Gallardo-Gaona JM, Ramírez-Calvo JA, et al. Amniotic band sequence: prenatal diagnosis, phenotype descriptions, and a proposal of a new classification based on morphologic findings. Rev Invest Clin. 2013; 65: 300-306.
5. Martínez-Frías ML. Epidemiological characteristics of amniotic band sequence (ABS) and body wall complex (BWC): are they two different entities? Am J Med Genet. 1997; 73: 176-179.
6. Dyson RL, Pretorius DH, Budorick NE, Johnson DD, Sklansky MS, Cantrell CJ, et al. Three-dimensional ultrasound in the evaluation of fetal anomalies. Ultrasound Obstet Gynecol. 2000; 16: 321-328.
7. Hartung J, Bollmann R. Nonimmune Fetal Hydrops (NIHF). Merz E (ed). Ultrasound in Obstetrics and Gynecology. Vol. 1. Obstetrics. 2nd edition. Thieme, New York, 2013, 188-199.
8. Schlehe B, Elsässer M, Bosselmann S, Axt-Fliedner R, Sohn C, Kohl T. Complete chorioamniotic membrane separation with constrictive amniotic band sequence and partial extra-amniotic pregnancy: serial ultrasound documentation and successful fetoscopic intervention. J Perinatol. 2014; 34: 941-944.
9. Mathis J, Raio L, Baud D. Fetal laser therapy: applications in the management of fetal pathologies. Prenat Diagn. 2015; 35: 623-636.
10. Beck V, Lewi P, Gucciardo L, Devlieger R. Preterm prelabor rupture of membranes and fetal survival after minimally invasive fetal surgery: a systematic review of the literature. Fetal Diagn Ther. 2012; 31: 1-9.
11. Chauhan SP, Scardo JA, Hayes E, Abuhamad AZ, Berghella V. Twins: prevalence, problems, and preterm births. Am J Obstet Gynecol. 2010; 203: 305-315.
12. Alvarado EA, Pacheco RP, Alderete FG, Luís JA, de la Cruz AA, Quintana LO. Selective termination in dichorionic twins discordant for congenital defect. Eur J Obstet Gynecol Reprod Biol. 2012; 161: 8-11.
13. Lynch L, Berkowitz RL, Stone J, Alvarez M, Lapinski R. Preterm delivery after selective termination in twin pregnancies. Obstet Gynecol. 1996; 87: 366-369.
14. Eddleman KA, Stone JL, Lynch L, Berkowitz RL. Selective termination of anomalous fetuses in multifetal pregnancies: two hundred cases at a single center. Am J Obstet Gynecol. 2002; 187: 1168-1172.
15. Bigelow CA, Factor SH, Moshier E, Bianco A, Eddleman KA, Stone JL. Timing of and outcomes after selective termination of anomalous fetuses in dichorionic twin pregnancies. Prenat Diagn. 2014; 34: 1320-1325.