LETTER
Hippokratia 2021, 25(2): 97
Tryfon S1, Papadopoulou E1, Chatzis C2
1Pulmonary Department, General Hospital “G. Papanikolaou”, Thessaloniki, Greece, 2Primary Health Center, N. Madytos, Greece
![]()
Keywords: Orthopnea, dyspnea, bilateral hernia, Morgagni hernia
Corresponding author: Stavros M. Tryfon. General Hospital “G. Papanikolaou”, Thessaloniki, Greece, e-mail: stavrostryfon@yahoo.gr
Dear Editor,
Dyspnea is a common symptom indicating a plethora of different diseases, mainly heart or lung diseases, but may constitute the presentation of unexpected causes, such as chest wall or subdiaphragmatic disorders. Chest X-ray plays a pivotal role in the differential diagnosis of dyspnea and sometimes reveals surprising findings. We present an intriguing clinical case, highlighting the challenges in the differential diagnosis of severe dyspnea.
A 72-year-old female presented at the outpatient pulmonary department complaining of severe orthopnea and postprandial cough that obligated her to sleep in an upright position and persisted for one year. Her medical history included only arterial hypertension, for which she was treated with amlodipine (10 mg/day). Her clinical examination was unremarkable, and laboratory tests were within normal values.
Chest X-ray at first glance showed an air-fluid level in the left side, which resembled a cavitary lesion of the left middle lung field, whereas, on the right side, there was a pericardial round-shaped lesion containing air (Figure 1). Such findings, along with the patient’s clinical symptoms, were even more confounding. However, meticulous observation of the chest X-ray revealed a surprising diagnosis, namely a bilateral diaphragmatic hernia that exerted extreme pressure in the main bronchi. Specifically, the ascending colon and part of the transverse colon protruded into the thoracic cavity on the right side and the stomach on the left side (Figure 2). Despite the severity of her symptoms, the patient was unwilling to undergo any interventional procedure or CT-scan imaging.
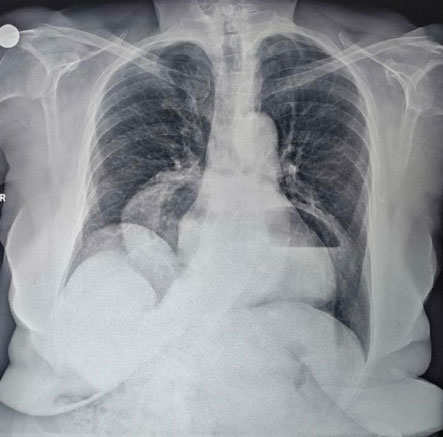
Figure 1: Chest X-ray depicting an air-fluid level on the left side and a round lesion containing air on the right side.

Figure 2: Drawing on the chest X-ray of the bilateral diaphragmatic hernia’s contents, with the ascending colon and part of the transverse colon protruding into the thoracic cavity on the right side ( solid white arrows), and the stomach on the left side ( semisolid white arrows).
This case highlights the clinical challenges of diagnosing Morgagni hernias in Primary Health Care. Depending on its contents (i.e., omentum, stomach, small intestine, liver), Morgagni hernia mimicks different pathological entities and appears differently on chest radiography, which may result in misdiagnosis. The differential diagnosis comprises of intrathoracic tumors, atelectasis, pneumonia, and pericardial cysts1.
Morgagni hernias are located in approximately 90 % of patients on the right side, 2 % on the left, and 8 % bilaterally2. Usually, during infancy and childhood, they remain asymptomatic but may progressively enlarge in adulthood and become symptomatic due to the increased intra-abdominal pressure3. Such an extensive bilateral diaphragmatic hernia manifesting with severe orthopnea in an elderly woman, as in this case, poses a clinical challenge due to its rarity and clinical presentation. Meticulous observation of the chest X-ray sufficed to establish a diagnosis in this case, but computed tomography scan serves as an accurate, non-invasive method in challenging cases of Morgagni hernias. Further diagnostic assessment for the exclusion of a potential underlying intra-abdominal pathology resulting in such a hernia should be undertaken.
Conflict of interest
The authors disclose no conflict of interest.
References
1. Svetanoff WJ, Rentea RM. Morgagni Hernia. StatPearls Publishing, Treasure Island, Florida. 2021. Available at: https://www.ncbi.nlm.nih.gov/books/NBK557501, date accessed: 02/06/2021.
2. Federico JA, Ponn RB. Foramen of Morgagni hernia. Shields TW, LoCicero J III, Ponn RB (eds). General Thoracic Surgery. 5th Edition. Lippincott Williams & Wilkins, Philadelphia, 2000, 647-660.
3. O’Brien C, Jobling JC. Symptomatic bilateral Morgagni diaphragmatic hernias in an elderly patient. BJR Case Rep. 2017; 3: 20160110.